India Toolkit: Advocacy
Using Data to Effectively Manage the Family Planning Program
 Purpose: This tool helps in monitoring the performance of Family Planning (FP) strategies as per the Expected Level of Achievement (ELA) by analyzing relevant indicators and thus enabling timely corrective measures and allowing data use in decision-making to meet the FP objectives of the district and the state.
Purpose: This tool helps in monitoring the performance of Family Planning (FP) strategies as per the Expected Level of Achievement (ELA) by analyzing relevant indicators and thus enabling timely corrective measures and allowing data use in decision-making to meet the FP objectives of the district and the state.
Audience:
- Additional Director / Joint Director (AD/JD)
- General Manager-FP and Urban
- Chief Medical Officers (CMO)/Additional Chief Medical Officers (ACMO)
- Chief Medical Superintendent (CMS)
- Divisional Urban Health Consultant (DUHC)/District Program Managers (DPM)
- Urban Health Coordinator (UHC)
- HMIS Manager/FPLMIS Manager
- City Community Process Managers (CCPM)
- Medical Officers In-charge/ Private facility In-charge
- Assistant Research Officers (ARO)/ Data Entry Operators
Background: The Ministry of Health and Family Welfare’s (MoHFW) routine Health Management Information System (HMIS) captures various data related to FP. In addition, the private sector reports FP data to the government via different mechanisms. However, there are issues in data management such as facilities not reporting on FP in the HMIS; incomplete reporting formats being filled; inconsistencies such as IUCD and sterilization data being reported from facilities where services are not available due to lack of trained providers, equipment, supplies and necessary infrastructure to conduct procedure etc. In addition, the available urban FP data is not routinely collated, validated, fully analyzed or presented in a manner that can help the district level officials, managers, hospital administrators or providers in understanding the current performance or in taking programmatic decisions, based on the understanding of relationship between unmet need and available resources for FP across both government and private sector facilities. Only when the data is analyzed and discussed in various review meetings, can it inform decisions for taking corrective measures timely and encourage good performance.
The TCI tutorial below features a webinar held in May 2020 showcasing TCI’s data management solution.
Evidence of Effectiveness
TCI India technically assisted government officials of 20 cities of Uttar Pradesh (UP) on the regular review and monitoring of HMIS data for taking timely decisions. The changes in FP annual client volume at the district, city and UPHC level was analyzed and how UPHCs contributed (or not) to the overall FP acceptors in the district was thoroughly reviewed by the government. Hence, evaluation of HMIS trend by city, by district, by UPHC, and by month through near-real-time data became a practice. The government officials along with TCI India reviewed data at each level and accordingly formulated the coaching, mentoring and implementation plan for the cities.
The HMIS data trend helped the UP government to understand the importance of TCI coaching mentoring model behind the improved performance of 27% cities (20 intervention cities) in comparison to the remaining 73% cities (55 non-intervention cities) of the state, and this provided evidence for scaling up TCI India’s high impact approaches (HIAs) in non-intervention cities in UP. (refer to the trend graph below)
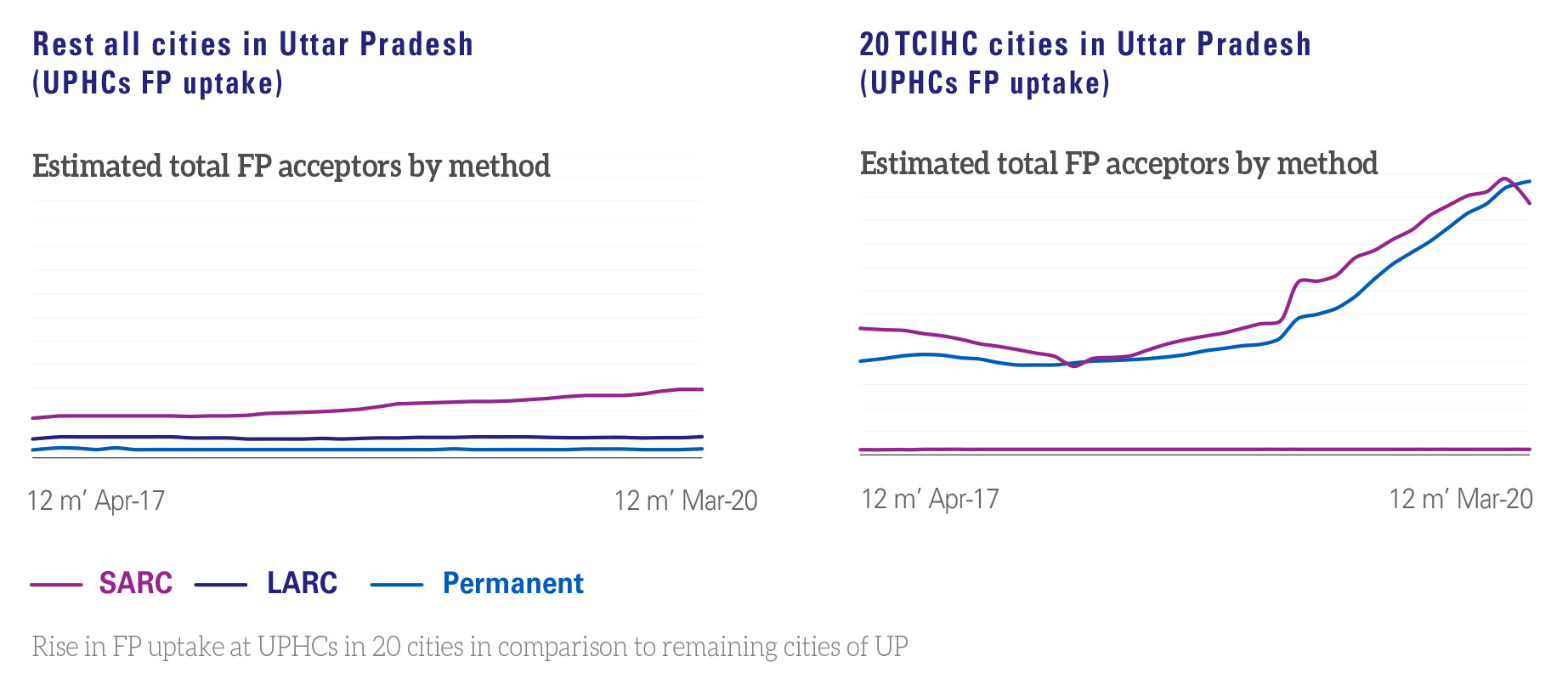
The reversing trend in UPHCs of TCI India supported cities annual client volume for Short-Acting Reversible Contraceptive (SARC) and Long-Acting Reversible Contraceptive (LARC) is visible with great significance, while in remaining cities the trend is diminishing especially for IUCD and stagnant for other methods. The contribution of IUCD in method mix is significant in TCI India cities and its contribution is also positive in city-level achievements. On the other hand, data from the remaining cities in UP reveals a total of 19,139 number of annual client volume in April 2017, which reached 32,397 number with 69% increase in March 2020. Additionally, there is a small increase recorded at UPHCs for SRAC (condoms, DMPA and oral contraceptive pills) and largely no change recorded in IUCD client volume in non TCIHC supported cities.
In March 2017 these 20 cities recorded 105,763 annual client volume which reached 229,793 numbers in March 2020. It also recorded an 119% increase in client volume. Particularly, IUCD, injectable, condoms and pills.
TCI India experience showed that the use of data for program management could be a powerful and a low-cost means to improve access, quality of services, provider’s motivation and accountability. FP performance improved when available data was analyzed routinely (presented through simple line graphs and bar charts) in review meetings headed by AD/CMO and was utilized to inform progress of urban FP strategies against ELA over the given period. By reviewing and discussing the monthly program achievements and the trends over time, health officials were able to identify specific problems requiring attention and were able to take corrective actions including re-allocation of human and other resources to address these problems. Furthermore, the routine review of data in these meetings led to increased visibility, attention and priority was given to the urban FP program in in general.
Data on urban FP indicators presented by TCI India supported cities at division level review meetings triggered an interest at the division level to scale up high impact approaches (HIAs). This interest lead to the division head, AD seek TCI India’s coaching on scale-up of HIAs to cities in the division not supported by TCI; the cities include Mainpuri (Aligarh), Kasganj (Agra), Deoria (Gorakhpur), Orai/Jalaun (Jhansi), Unnao (Kanpur), Raebareli (Lucknow), Baghpat (Meerut), Sambhal (Moradabad), Fatehpur (Allahabad), Bareilly (Badaun) and Chandauli (Varanasi). Each of these cities were coached by master coaches (selected government officials from the system) of the TCI India supported sites in the same division, for example Mainpuri was coached by master coaches from Aligarh. Thus, in line with the cascade coaching model master coaches, coached city UHC on formation and regularization of convergence platform to roll out fixed day static service (FDS)/Antral diwas, build capacities of Urban ASHAs and regular data reporting and review initiated. These eleven cities started conducting FDS/Antral diwas and reported FDS data in the HMIS; a never before activity done by any of these cities.
Guidance on Improving the Urban Slum Population Database
The key to effective data management leading to better program decision-making includes following steps:
1. Determine the indicators
Determining the FP indicators that need to be captured is an essential step. This should be based on the goals of program or questions/issues that need to be addressed to strengthen FP program of the city. For example: Are we reaching clients in need of family planning services? Are resources adequate to maintain quality of care? Depending on the goal or question, identify appropriate indicators, such as number of clients that received a family planning method disaggregated by age or percentage of facilities with LARC in stock.
2. Make operational definition of indicators
To build a common understanding on the indicators the numerator and denominator should be clearly defined, if necessary, can be explained by giving examples.
3. Finalize source and frequency of data collection
The indicators must be finalized together with their source (points of data collection) and frequency (timelines for collecting different sets of data). For example, an indicator like the number of clients provided different FP method can be collected from facilities on monthly basis. The data reporting date should be monitored as this will help in streamlining timely reporting from different sources.
4. Devise Expected Level of Achievements (ELAs)
Without giving any target in terms of number of clients for different FP methods, ELAs must be finalized, because in FP program providing informed choice to eligible couple is most essential. The ELAs can be collectively decided with stakeholders by considering data for previous years and unmet FP need (total and for spacing method) of the people.
5. Coach staff on use of data
All the staff handling data should be informed and coached on all the data forms, the definitions of key indicators and the basic analysis of the data and indicators. Annual training/ refresher training on data management must be considered and funds to be made available through the Program Implementation Plan (PIP). Master trainers/coach can be identified by the CMO at the city level.
6. Validate data to improve data quality
At the UPHC level data validation committee must be formed and each month prior to HMIS data reporting committee must conduct a meeting to check data and rectify errors. At the district level data of facilities to be validated, and district level meeting to be conducted with in-charge of facilities to resolve data related issues such as error in data, over/under reporting and delay in reporting.
7. Using data for feedback
While it is important for the district health teams, facility-in-charges, and Auxiliary Nurse Midwife (ANM) to review the available data and reports and take corrective actions on the basis of identified gaps and weaknesses; it is equally important to communicate the gaps to the team in a positive manner so that it boosts their morale and yet provides direction for course correction.
A simple way of doing this is to appreciate and acknowledge each person right in the beginning, followed by suggested improvement (including offering any support/ peer coaching that the person may require) instead of direct blaming, public shaming as it actually demotivates people.
Important points on use of data
- Key FP indicators should be reviewed and discussed in monthly and key review meetings (District Health Society/FP/NUHM review meeting) by the CMO and concerned authorities (Nodal officers, UHC, MOIC, etc.)
- Line and bar graphs should be produced and displayed each month and also at the end of each year in the district health offices and facilities.
- Feedback including bar charts and graphs showing comparative performance and performance-over-time should be provided to all the facilities
- Feedback and supportive supervision using data should be provided to individual staff from their supervisors at every level
Roles and Responsibilities towards Data Usage for Program Management
AD/JD/General Manager FP and Urban
- Include urban FP data review as an agenda in all types of review meetings.
- Issue guidance to all the cities to refer this tool as one of the guidance documents to utilize data effectively for strengthening urban FP program.
CMO/ACMO
- Ensure that facilities report data on a regular and timely basis as per the defined data flow process
- Ensure that all the staff responsible for data management has been appropriately trained, and if required, provide refresher training
- Share the standard template for monthly reporting and reviewing key FP indicators at the district level (facility wise, method-wise and month-wise analysis)
- Ensure provision of funds for review meetings and training of staff on data management is available in the PIP Ensure usage of data during regular supportive supervision visits by nodal officers, ACMOs, DPMs, CCPM for supporting providers, UHC and facilities towards improving the performance
- Recognize high performers and give constructive feedback to others for programmatic improvement
- Urge private sector facilities to report data on agreed indicators on FP services which they provide for HMIS upload
- Issue directives for the formation and regular meeting of data validation committee at the UPHC level
- Issue directive to facilities where errors in data reports are consistent
- Issue directives to facilities which are low performing in providing FP services
CMS/DUHC/Nodal Officer- Urban Health and Family Planning
- Review the performance of providers on services provided in the facility (method-wise and month-wise)
- Review the post-partum and post-abortion FP data against institutional deliveries and clinical abortions respectively
- Give constructive feedback to providers to rectify identified problems and support them to improve
Medical Officer in-Charge (MoIC)
- Collect and collate data from ANMs and UPHC and review it to ensure its completeness and accuracy before reporting to HMIS
- Review performance of ASHAs in periodic ASHA and ANM meeting.
- Based on data give constructive feedback to the UPHC staff, ANMs and ASHAs to rectify identified problems and support them to improve.
- Ensure data validation committee meetings are regularly held and decisions taken are adhered to rectify data errors and improve data quality
- Ensure data is timely collected, collated and validated for HMIS upload.
CCPM
- Ensure capacity building of ASHAs and ANM on data reporting
- In coordination with MOIC, conduct periodic review of ASHAs’ performance on family planning indicators
ANM
- Coach ASHAs to plan household visits based on the data and report to the appropriate higher official
- Coach ASHAs to maintain daily field visit report in the urban health index register/specified reporting format
- Report every month on the given indicators such as number of clients who obtained FP services from public and private sector
Monitoring the Usage of FP Data for Program Management
Monitoring of data usage for program management should be based on the following indicators:
1. Activities | HMIS | For indicators 3-9 monthly facility/service delivery point report
- Percentage of facilities/ service delivery points (public and private) reporting in the HMIS
- Percentage of facilities/ service delivery points (public and private) reporting on FP indicators in HMIS
- Number and percentage of FP acceptors, by method, by facility (public and private)
- Method-specific percentages of all FP acceptors by facility
- Number of Fixed Day Static (FDS) service days, by facility
- Number of clients served per FDS
- Number of new FP acceptors mobilized by ASHA
- Number and percentage of Post-Partum Family Planning (PPFP) acceptors, by method
- Number and percentage of Post-Abortion Family Planning (PAFP) acceptors, by method, by facility
- Number of service providers inserting IUCD and administering injectable contraceptive
2. Human Resources | Monthly facility report
- Percentage of staff positions filled against those planned (reported and reviewed quarterly)
- Doctors trained on NSV / minilap, facility-wise
- UPHC-doctors, staff, nurses, ANMs, FP counselors, ASHAs
3. Training/Capacity building | Training database updated periodically
- Number of trained staff as reported by the facility (reported and reviewed periodically)
- Number of trained NSV surgeons
- Number of trained staff nurses/ANMs in PPIUCD
- Number of trained doctors in minilap/laparoscopic female sterilization
- Number of trained ASHAs on FP
- Number of trained doctors/staff nurses on new contraceptive methods
4. Budget | District monthly fiscal report
- Percentage of funds utilized against funds budgeted, by the city (reported and reviewed monthly and annually)
5. Accreditation | For UP- Hausala Sajheedari dashboard | For other states- Monthly report for Dept. of Health
- Number of accredited facilities with various government schemes
6. Commodities and equipment | Monthly facility indenting format and FPLMIS portal
- Contraceptive stockouts by method, by month and by facility (reported and reviewed monthly and annually)
- Equipment available and functional against planned
- Kelly’s forceps
- IUCD kit
- NSV kit
- Mini lap kit
- Laproscope
- Online indenting done by UPHC staff and ASHAs on FPLMIS portal
Cost Elements
The following cost elements are required for an effective data usage and management system. Their PIP codes are provided below for easy reference. A state may already have these elements, but if not, then they should be budget-ed in the PIP.
This table is indicative and illustrates the manner in which cost elements are provided in a government PIP, thus giving guidance to the audience on where to look for elements related to a particular task, such as using data to effectively manage the FP program.
Sl. No. |
FMR Code |
Cost elements/PIP budget head |
| 146 | HSS (U.6) | Planning and Program Management (Review Meeting under NUHM , Planning and M&E) |
|
49 J |
RCH 6 | M& E- World Population Day and Vasectomy fortnight |
| 50 J | RCH 6 | M&E – Other Family Planning Components |
Source: NHM PIP Guideline 2022-2024
Sustainability
Routine HMIS provides the basic data, while the staff who enters the data and does the basic analysis is already in place. If the available data is analyzed and made part of the routine review process where people can see the benefit of analyzing data and using it to make necessary corrections/ adaptations, then the entire process of data collection, analysis and feedback will sustain.
TCI APP USERS PLEASE NOTE
You will only receive CERTIFICATES by email – when earning a score above 80% – and will not be able to view or print a certifcate PDF from the TCI app.
Test Your Knowledge
Earn a Certificate
Infographics

English |

Hindi |

English |

Hindi |

English |

Hindi |
Government of India Resources
- Health Management Information System (HMIS)
- NUHM reporting Format, March-2017
- Hausala Sajheedari
- ROP 2017-18, NHM-UP