
India Toolkit: Demand Generation
Strengthening Women’s Groups (Mahila Arogya Samitis)
Facilitating Access to Family Planning Services among the Urban Poor
 Purpose: This tool provides guidance on how to establish Mahila Arogya Samitis (MAS), build their capacity as health advocates and develop them into self-governing institutions that work towards addressing and meeting the health and family planning (FP) needs of the community.
Purpose: This tool provides guidance on how to establish Mahila Arogya Samitis (MAS), build their capacity as health advocates and develop them into self-governing institutions that work towards addressing and meeting the health and family planning (FP) needs of the community.
Audience:
- Additional Director/Joint Director
- General Manager-FP and Urban
- Chief Medical Officers (CMO)/Additional Chief Medical Officers (ACMO)
- Nodal Officer- Urban Health & Family Planning
- Divisional Urban Health Consultant (DUHC)
- District Program Managers (DPM)
- Urban Health Coordinators (UHC)
- District/ City Community Process Managers (DCPM/ CCPM)
- District Family Planning Logistics Management Information System (FPLMIS) Manager
- Medical Officer In-Charge – Urban Health Primary Center (UPHC)
- Auxiliary Nurse Midwives (ANMs)
- Non-Government Organizations (NGOs)/Health Partners
Background: Women groups can be effective in expanding the base of health promotion efforts at the community level and building sustainable community processes. For this reason, the National Urban Health Mission (NUHM) has made a long-term commitment to community empowerment and leadership within the community by creating a role for women’s groups in the form of MAS.
The NUHM guidelines (Refer to: Guidelines for ASHA and Mahila Arogya Samiti in the urban context by National Urban Health Mission – 2014, Page nos. 17 to 23) define MAS as a community group involved in community awareness, interpersonal communication, community-based monitoring and establishing linkages with services and referrals. This group focuses on preventive and promotive health care, facilitating access to identified facilities and management of untied fund. A key function of the MAS is to support community members to access health entitlements.
Evidence of Impact
Documented evidence from other countries demonstrates the impact of women groups on improving FP and maternal and new born health (Refer to: Post A. et.al., Women’s group practicing participatory learning and action to improve maternal and newborn health in low resource setting: a systematic review and meta-analysis, Lancet 2013, 381, page nos. 1736 to 1746).
Similarly, with the coaching and mentoring support of TCI India, the government officials of Uttar Pradesh utilized MASs to improve access to FP services across 25 cities. In these TCI India intervention cities, 40 percent of the 5113 active MAS received untied funds, out of which 70 percent MAS utilized untied funds. TCI India assisted government with FP training for 50% of MAS members across 29 cities, who then trained the remaining MAS members. After receiving training, these groups integrated family planning into their existing agenda. With the assistance of ASHAs, MAS worked to become a resource agency that disseminated family planning information to the community and supported eligible couples to access family planning services and entitlements provided under government schemes. Around 47% of MAS supported ASHAs in conducting Saas Beta Bahu Sammelan during World Population Day 2022 fortnight. Many women’s groups also worked to access entitlements for community members related to nutrition, routine immunization, neonatal care, etc.
“I informed a young woman Moni about family planning choices for spacing between children. However, her mother-in-law stopped her from adopting any family planning method. I tried counseling her mother-in-law, but she did not listen to me. Soon, I learnt that Moni was pregnant with her second child. After her second delivery, I spoke to Mahila Arogya Samiti members and requested them to counsel Moni’s mother-in-law so that she does not conceive yet again and get burdened. MAS members invited Moni and her mother-in-law in their next group meeting where they counseled both of them. Moni soon visited and met the UPHC doctor who explained the basket of choices to her and she availed a method of her choice”
Guidance on Establishing and Strengthening MAS
The steps below provide guidance on establishing and strengthening MASs

Identify Women Who Can Form a MAS
- As per guidelines, identify clusters of households where a MAS needs to be formed
- After conducting meetings at the community level in order to understand the health needs of the community, ASHA will sensitize the identified women on the role of MAS
- Women who consistently participate in these meetings will emerge as MAS members
- In slums, where other women groups such as self-help groups, savings groups etc. exist, these groups should be oriented by the ASHA, and members of these groups should be encouraged to join or form a MAS. These other groups can be co-opted into MAS, provided they-
- obtain approval from the respective authorizing department e.g. National Urban Livelihoods Mission (NULM), District Urban Development Agency (DUDA), Integrated Child Development Services (ICDS)
- open their membership to include new members and representation from all socio-economic sections
- incorporate health as a priority in their agenda
Selection of MAS Members
- Key criterion for selection of MAS members should be their commitment and willingness to work as a collective for community work.
- Inclusion of women from the poorest and most marginalized segments of the community in the MAS is critical as they have the least access to health information and services.
Build Capacity of MAS Members on Health Issues including FP
- Plan training on FP, MNCH for MAS members as budgeted in NHM
- Provide relevant IEC materials and job-aids including frequently asked questions
- Provide resources to MAS member for executing gender integration activities
- Provide support to MAS members through joint home visits and continue building capacity of MAS members on FP, inter-spousal communication to promote shared decision-making among couples and support for contraceptive use.
- Motivate them to use gender-inclusive language such as “people,” “folks,” or “individuals” in their daily communication instead of “women” etc.
- Coach MAS members to address cultural and social norms that impact gender equality by enhancing their skills on creating awareness on Pre-Conception and Pre-Natal Diagnostic Techniques (PCPNDT), promoting spousal communication, and increasing male participation in FP.
- Reinforce key issues such as including the most marginalized population groups, raising and using resources, undertaking advocacy etc.
- Provide opportunities for MAS members to present their issues before the District Health Society (DHS).
- Link MAS to the DUDA or to ICDS project officers
Use platforms such as World Population Day, World Contraceptive Day, Saas Beta Bahu Sammelan, Arogya Mela, or Breastfeeding Week to increase visibility and recognition for MAS. Such recognition strengthens and motivates the group.
Support Key MAS Activities
- Support ASHA in mapping and listing slum households and preparing resource maps in the communities.
- Monitor and facilitate access to essential public services related to health, water, sanitation, nutrition and education.
- Support ASHA, Anganwadi Workers (AWWs) and Auxiliary Nurse Midwives (ANMs) in organizing Urban Health and Nutrition Days (UHNDs), and in mobilizing women, adolescents, and children for outreach sessions.
- Generate demand for health services, including FP.
- Refer eligible couples to Fixed day static service (FDS)/Antral diwas.
- Support ASHAs to create awareness regarding gender issues such as PCPNDT, spousal communication, male participation in RCH etc.
- Support in gender integration activities or simulation games, for example interactive games to change the mind-set of son preference in the community (white and black marble game), Kranti Bhranti an interactive game of Rashtriya Kishore Swasthya Karyakram (RKSK)
- Support ASHA in counseling family members on health issues, promoting spousal communication on FP and identifying gender champions from the community.
- Encourage couples to be smart in planning their families, maintaining appropriate space between children and mutually agreeing on adopting a family planning method.
- Ensure access to health entitlements for the community.
- Ensure community access to health facilities, including accompanying women whenever required.
- Lead collective action and self-help initiatives at the community level.
- Support ASHAs and AWWs in the distribution of health supplies, including FP methods. They can also be depot holders for condoms, OCPs, ORS etc.
- Use untied funds to address the health needs of the community.
- Participate in health campaigns, special events and drives
Roles and Responsibilities towards strengthening Mahila Arogya Samitis
Role |
Responsibility |
General Manager FP/Urban/JD/AD |
|
CMO/ACMO |
|
Nodal Officer – Urban Health |
|
District Program Managers, Urban Health Coordinator, Community Process Managers |
|
Medical Officer In-Charge – UPHC |
Ensure that ASHAs are performing the following activities to form and strengthen the MAS:
|
ANM |
|
Monitoring MAS Activities in Family Planning
As per NUHM guidelines, the monitoring of MAS and related reporting by ASHAs / ASHA facilitators to the CMO should include the following indicators:
- Number of MAS established
- Number and percentage of MAS that received FP trainings
- Number of MAS that received untied funds
- Number of MAS utilizing untied funds as per guidelines
- Number of UHNDs and outreach camps supported by MAS members as compared to the total number of UHNDs and camps conducted
- Qualitative analysis of the sample agenda/ minutes could also be done to overview compliance
- Number of MAS meetings where gender integration discussions held or simulation games utilized
Cost Elements
This table is indicative and illustrates the manner in which cost elements are provided in a government Program Implementation Plan (PIP), thus giving guidance to the audience on where to look for elements related to MAS.
| Cost Element | FMR Code |
| Orientation of MAS members | HSS(U).2.131- MAS |
| Untied Fund | HSS(U).9.149.UG.3 (Untied Fund to MAS) |
* Source: NHM PIP Guideline 2022-2024
Sustainability
Creating sustainability for MAS is a long-term process, which requires on-going training and supportive supervision by ASHAs and other health functionaries. It also requires linkages to various income generation schemes of the government as well as the annual budget provisioning through the PIP. Reward and recognition to well performing MAS can provide motivation for their continued involvement.
TCI APP USERS PLEASE NOTE
You will only receive CERTIFICATES by email – when earning a score above 80% – and will not be able to view or print a certifcate PDF from the TCI app.
Test Your Knowledge
Earn a Certificate
Available Resources
- Guidelines for ASHA and Mahila Arogya Samiti in the Urban Context by National Urban Health Mission, Page No. 17 to 23
- Induction for Mahila Arogya Samiti_English
- Induction for Mahila Arogya Samiti_Hindi
- Contraceptives Display Kit
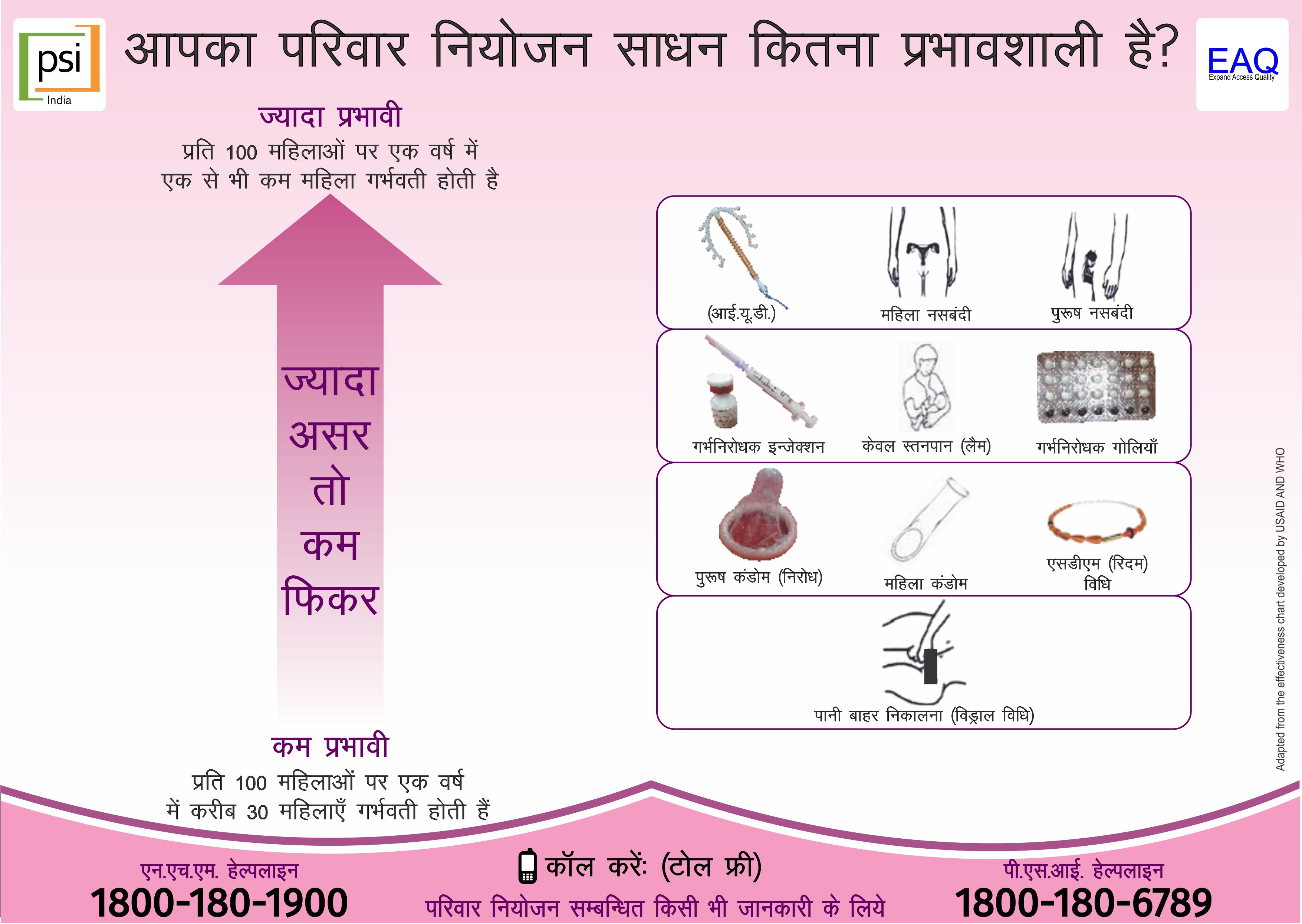
- Family planning effectiveness chart
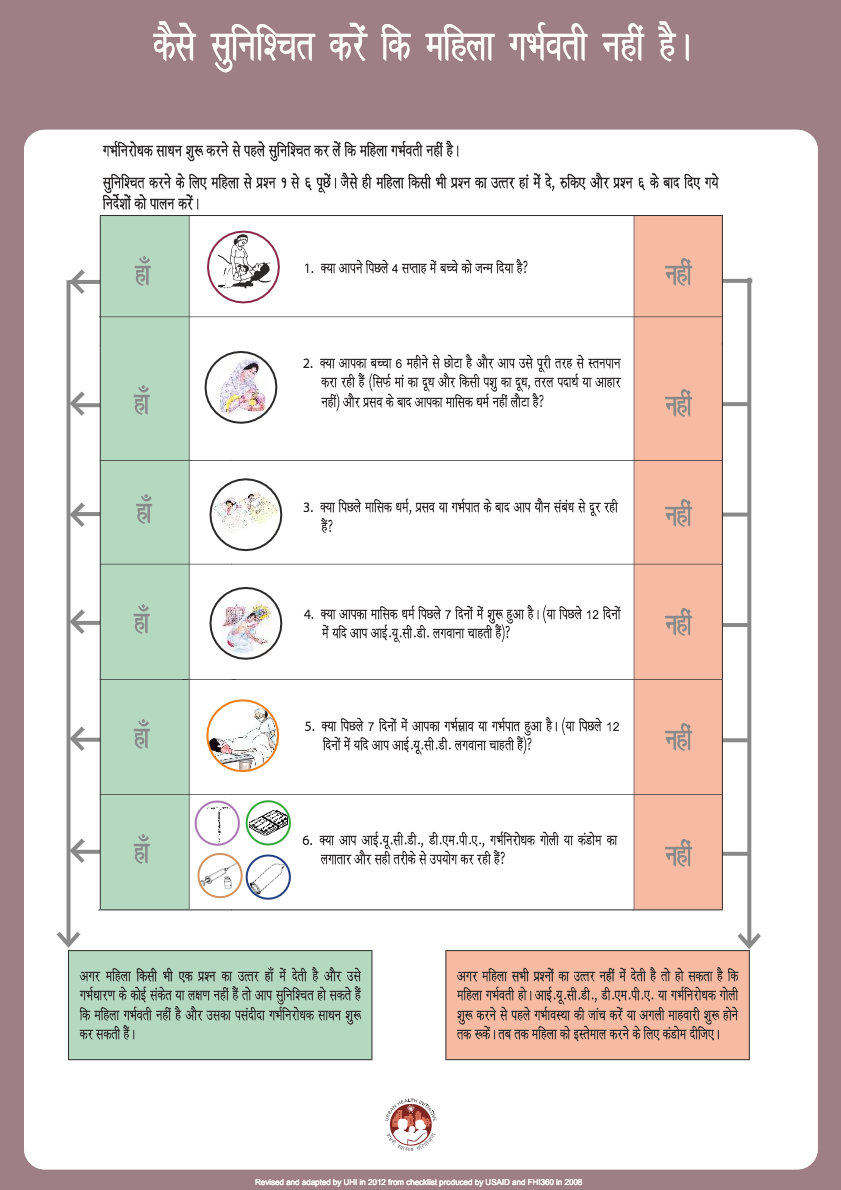
- Pregnancy screening checklist
- Orientation module for planners, implementers and partners, Section 4 point one, page no 53-62
- TG segmentation matrix
- Method Specific Training PPTs
- Method Specific counseling cards
- Frequently Asked Questions and Answers
- RKSK Kranti Bhranti -Interactive Game
- Women’s Group Practicing Participatory Learning and Action to Improve Maternal and Newborn Health in Low Resource Setting: A Systematic Review and Meta-analysis, Lancet 2013, 381, Page No. 1736 to 1746
- NHM PIP guideline for a particular financial year
- TCI India Fixed Day Static Approach to Expand Access to Quality Family Planning Services approach
- TCI India Mapping & Listing of Urban Slums approach
- TCI India Enabling Urban Accredited Social Health Activists approach
- Strengthening the Linkages Between Community Structures and the Health System in Moradabad, Uttar Pradesh

{kind=link}
{kind=link}
{kind=link}