Background

A NURHI-designed market umbrella promotes family planning at a market in Ilorin in the central state of Kwara. Image Credits: Akintunde Akinleye, 2012.
The most populous country in Africa, Nigeria’s urban growth rate is 3.75%, compared to an overall growth rate of 2.5%, with over half of its population living in urban areas. Contraceptive use is typically higher and fertility levels lower in urban areas, as compared to rural areas. However, contraceptive use is often not equally distributed among all urban residents; evidence suggests significant disparities in fertility rates and contraceptive use behaviors among urban wealth quintiles. In Nigeria, the fertility rate is higher among the urban poor as compared to the urban rich. Knowledge and use of modern contraception also increase with greater household wealth.
 Both the public and private sectors in urban areas are important to ensure equal access to family planning (FP) services and the availability of modern contraceptive methods. Because neither sector in Nigeria had been analyzed regarding access to and availability of FP services by the different subpopulations of wealth status, it was not known whether public or private sector facilities were effectively serving the urban poor. This study fills an important gap in knowledge about Nigeria’s contraceptive supply environment. Using survey data from FP service delivery points (SDP; hereafter facilities), supply index scores (SIS; hereafter scores) were created to measure the aggregate-level public and private sector FP supply environment in and across six selected cities.
Both the public and private sectors in urban areas are important to ensure equal access to family planning (FP) services and the availability of modern contraceptive methods. Because neither sector in Nigeria had been analyzed regarding access to and availability of FP services by the different subpopulations of wealth status, it was not known whether public or private sector facilities were effectively serving the urban poor. This study fills an important gap in knowledge about Nigeria’s contraceptive supply environment. Using survey data from FP service delivery points (SDP; hereafter facilities), supply index scores (SIS; hereafter scores) were created to measure the aggregate-level public and private sector FP supply environment in and across six selected cities.
The study addressed the following issues:
- Whether the public and private sector FP supply environments were consistent across urban areas, and if not, how they differed.
- Whether and how services provided in one sector were associated with and/or complimented services provided in the other sector.
- FP supply was defined as product availability and access to contraceptive services. The study considered “availability” as whether contraceptive commodities were actually on hand and could be obtained at any given facility. “Access” was defined as the degree to which FP services could be obtained by a large majority of the population.
- By linking aggregate-level facility data with data collected at the same time from individuals living in corresponding communities, the study explored whether the FP supply environment was associated with community-level wealth status, and whether services were distributed in a way that might lessen barriers to contraceptive access and availability among the urban poor.
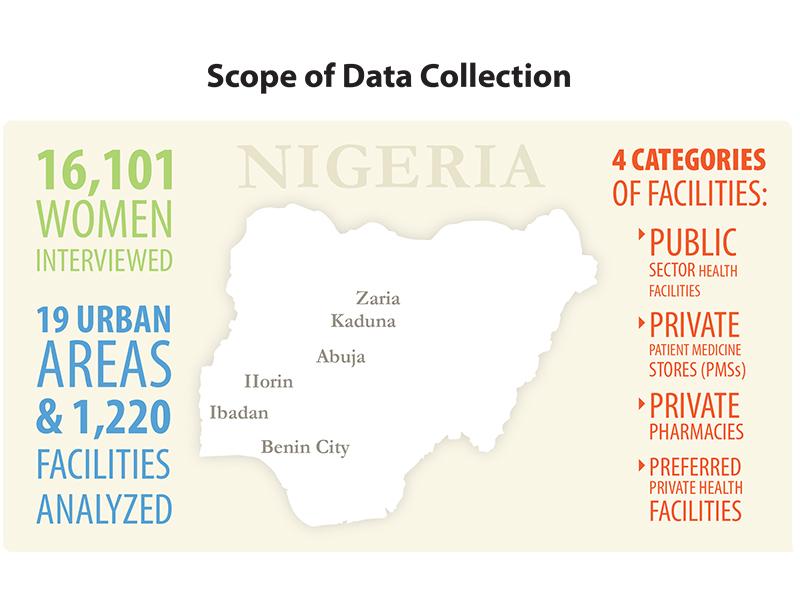
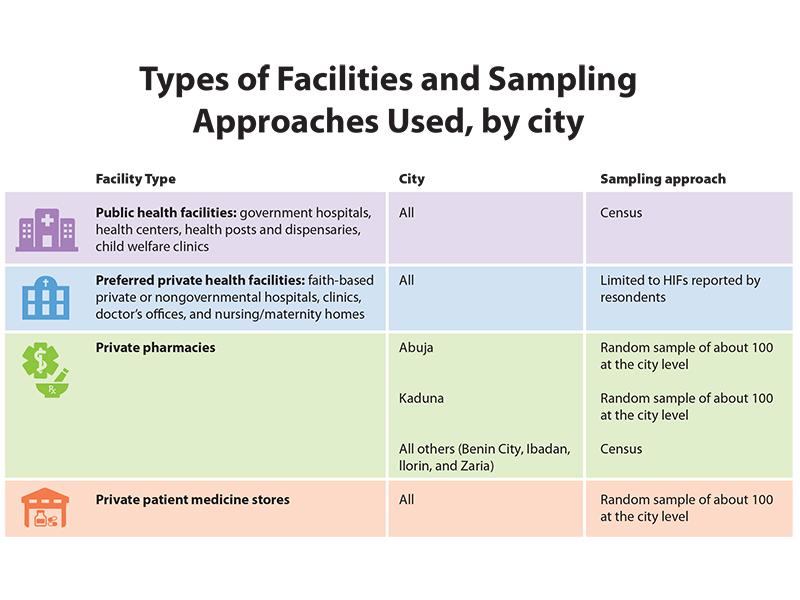
Individual and facility data were collected at baseline from six cities (Abuja, Benin City, Ibadan, Ilorin, Kaduna and Zaria) and 19 local government areas (LGA). Nigeria is divided into states, which are subdivided into LGAs. This study looked at the urban portions of the LGAs that lie in the six selected cities. Information obtained from 16,101 women interviewed in the 19 urban areas and from 1,220 facilities were analyzed. Four categories of facilities were included: (1) public sector health facilities; (2) preferred private health facilities; (3) private pharmacies; and (4) private patent medicine stores (PMSs). The various types of facilities and the approach used to sample them are described in the graphic.
Access to FP is contingent on the consistent and convenient availability of contraceptive methods.
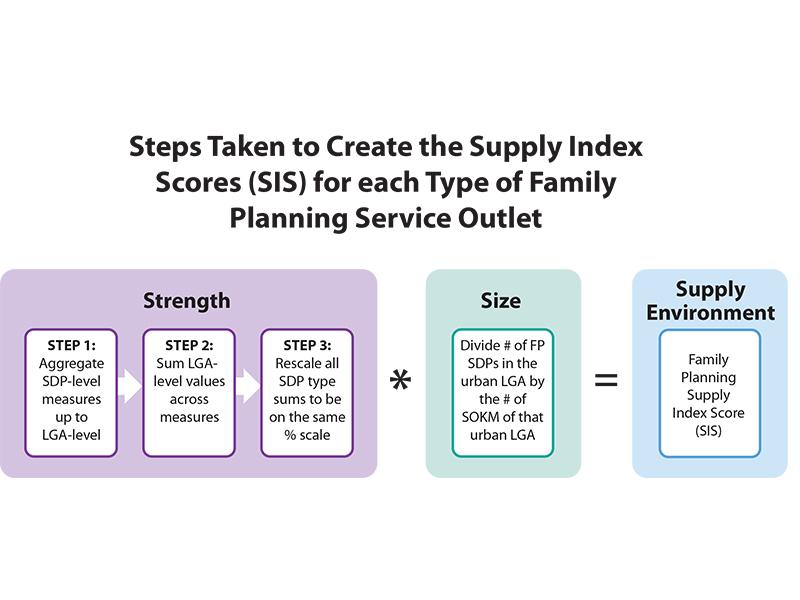
Two important components of contraceptive access and availability were used to define the aggregate-level FP supply environment and determine the supply index scores: the overall strength of FP supply among the facilities in each LGA and the density of facilities that provide FP in each area.

Results
Strength of FP supply: The average strength of FP supply scores among the different types of facilities were low, with little variation between the public and private sectors. This implies that a substantial percentage of facilities in each LGA either: (1) did not offer all the contraceptive methods that should normally be available in each type of facility; (2) experienced commodity stock-outs; (3) were not open for the maximum number of hours per week; (4) did not offer socially marketed products; and/or (5) required partner consent to obtain at least one available method (not including sterilization). For example, among the public and preferred private sector facilities, the elements that increased the scores were the number of hours that the facilities were open and the percentage that sold intrauterine devices (IUDs) and injectables. The overall scores for public and preferred private facilities were brought down because a large percentage in each of the 19 urban areas required partner consent for reversible modern contraceptive methods.
On average, 60.4% of public and 76.1% of preferred private facilities required partner consent for at least one available reversible contraceptive method.
Density of facilities: Although there was no discernible pattern across the areas surveyed, the average density of pharmacies and PMSs was far greater than that for public and preferred private facilities. In this case, the data showed wide variability in the density of public and preferred private facilities across the urban LGAs. The density of PMSs that carry contraceptives varied the most across LGAs, with the minimum number of PMS facilities per 100km2 being 13 and the maximum being 498. Where there was a good public sector FP supply environment, there was increased likelihood that there was also a good private sector FP supply environment. This result could reflect greater demand for all health services and thus more providers in those urban areas. However, there was not a significant association between the size of the urban LGA population and the density of providers, so another interpretation of this finding is that neither sector is working to address gaps in service delivery. Therefore, access to modern contraception could be improved if the government increased public FP facilities in areas that lack private facilities.
Access to modern contraception could be improved if the government increased public FP facilities in areas that lack private facilities.
FP supply environment and community-level wealth status: The data show that the level of public and private sector contraceptive access and availability are not associated with the location of the poorest women in each city. People who are poor are just as likely to live in a good FP supply environment as those who are wealthy, depending on the city in which they live. This result likely indicates that the FP supply environment serves needs that are not wealth-based.
Programmatic Implications

A patent medicine vendor, Chief Stephen-Kola Adewunmi, counsels a client, Lasisi Iyanda Hamed, in his shop. On display are materials promoting Nigerian Urban Reproductive Health Initiative (NURHI). Image Credits: Akintunde Akinleye, 2012.
This study provides sound baseline measures of the strength and size of the private and public FP supply environments in urban Nigeria. It identifies urban areas that have a weaker supply environment and compares those areas in which the urban poor are located. Although no systematic pattern was found between the private and public FP supply environment and urban poverty, program planners and policy makers can use the information to identify specific geographic areas and opportunities to encourage private sector expansion and/or redistribution of public services in highly concentrated poor areas that also have poor access to and availability of FP.
This story was originally written by the Measurement, Learning & Evaluation Project, which evaluated the Urban Reproductive Health Initiatives (UHRIs) in Kenya, Senegal, Nigeria and India. The Challenge Initiative is charged with expanding access to the proven solutions and successes developed under the UHRIs.
