New Journal Article on TCI’s AYSRH Program Focuses on Its 4-Ringed Concentric Circle Framework
The Challenge Initiative (TCI) has just published a peer-reviewed article in Frontiers in Global Women’s Health that describes its adolescent and youth sexual and reproductive health (AYSRH) program and its initial success in using TCI’s RAISE Tool to assess progress towards self-reliance and sustainability in 39 supported cities* in Benin, India, Kenya, Nigeria, Senegal, Tanzania and Uganda.
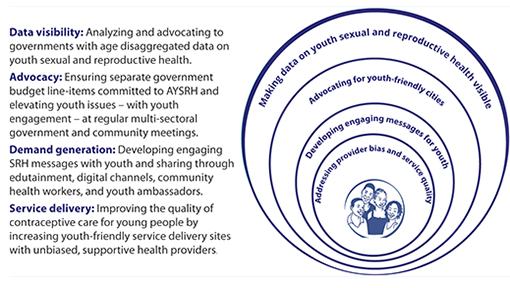
TCI’s four-ringed concentric circle framework for AYSRH programming.
The article is organized around TCI’s four-ringed concentric circle framework for implementing quality AYSRH programs and providing access to contraception for urban youth. The framework’s top priority is the importance of making AYSRH data visible to decision-makers, community members, and youth themselves. Next, it highlights the importance of youth engagement with government and community leaders to advocate for youth sexual and reproductive health (SRH) issues including funding.
The third ring emphasizes segmented demand generation messages for youth and their influencers (i.e., partners, parents, teachers, and other gatekeepers) through both interpersonal communication, WhatsApp chatrooms, and media channels. And central to the framework is addressing provider bias and service quality so youth are linked to quality AYSRH services delivered by sensitized facility staff oriented to set aside their biases against contraceptive provision – in particular for unmarried youth.
The third ring emphasizes segmented demand generation messages for youth and their influencers (i.e., partners, parents, teachers, and other gatekeepers) through both interpersonal communication, WhatsApp chatrooms, and media channels. And central to the framework is addressing provider bias and service quality so youth are linked to quality AYSRH services delivered by sensitized facility staff oriented to set aside their biases against contraceptive provision – in particular for unmarried youth.
The article notes that more than half of all adolescents globally live in Asia, with India having the largest adolescent population in the world at 253 million. In sub-Saharan Africa, adolescents make up the greatest proportion of the population, with 23% of the population aged 10–19. And these numbers are predicted to grow rapidly—particularly in urban areas as rural youth migrate to cities for economic opportunities. While adolescents and youth are subject to high sexual and reproductive health risks, few efforts have been documented for addressing these in urban settings, especially in poor settlements.
TCI’s demand-driven platform for sustainable scale and impact lets city governments—in particular urban slums—lead the implementation of its high-impact interventions for both family planning and AYSRH. In June 2018, TCI received additional support from the Bill & Melinda Gates Foundation to heighten its focus on AYSRH for youth living in urban slums. TCI dedicates technical and program support to married (including first-time parents) and unmarried youth ages 15–24 years. Using an innovative coaching model and an online learning platform (TCI University), TCI supports city governments as they implement AYSRH interventions to accelerate the impact of TCI’s model for rapid scale.
According to the article, TCI has been assessing the performance of cities implementing its AYSRH approaches using the RAISE tool and has found considerable improvement over two rounds of assessments through TCI coaching and support for adaptation of the high-impact interventions between the first and second round.
Invisible No More
Activating the Urban Health System to Deliver Quality Adolescent- and Youth-Friendly Health Services
TCI has also just published a booklet featuring highlights of its AYSRH work to accompany the Frontiers’ article.
KENYA
TANZANIA
UGANDA
SENEGAL
INDIA
NIGERIA
Round 2: 92%
Round 2: 89%
Round 2: 88%
Round 2: 74.5%
Round 2: 73%
Round 2: 69%
- Financial commitment for AYSRH
- Supportive supervision
- Coaching
- Community involvement
- Adolescent and youth-friendly services
- Advocacy
- TCI-U access and utilization
- Coaching
- Supportive supervision
- Public-private partnership
- Financial documentation and management
- Family planning and AYSRH strategies/approaches
- Coaching
- Supportive supervision
- Strengthened collaboration between municipality and health system
- AYSRH effectively layered onto TCI family planning program
- Strong landscaping to identify gaps and needs
- Strong political and health system commitment to AYSRH
- Improved leadership for AY interventions
- Youth participation in key meetings
- Review of AY program at city coordination committee meetings
- City leading AYFHS assessments
- Improved referral system
- Frontline health workers map and list adolescents and refer to UPHCs
- Advocacy for inclusion of AY indicators and data from HMIS in review meetings
- State adoption and scale up of best practices
- Increased social mobilization and referrals for AY services
- Improved provider behavior and increased availability of AYFHS
- Continuous political engagement
- Continuous advocacy for more resources
- Procure adequate tools
- Referral and linkages
- Follow up of coaches
- Avail and print guidelines for volunteers
- Use of FP champions for advocacy
- Enroll and orient more TCI-U users
- Conduct supportive supervision
- Partner with private sector, i.e., pharmacies and other NGOs providing FP/AYSRH services
- Non-technical coaching on financial management and documentation
- Disseminate family planning/AYSRH best practices at all levels
- Sisi-kwa-sisi coaching
- Supportive supervision
- Supportive supervision for AYSRH
- Implementation and monitoring of AYSRH best practices, including reduction of provider bias, whole-site orientation, comprehensive sexual education, home visits by community health workers, youth associations, social media and the transformational youth leaders
- Adolescent and youth-friendly checklist operationalized
- Management coaching facility staff for timely upload of AY data on HMIS portal
- Coaching LG to review data from facility and community at monthly review meetings
- Follow up of master coaches
- Re-stock and supplies (condoms, OCP and EC)
- Supportive supervision of AY counsellors at District Hospitals and District Women’s Hospitals
- Partnership with private sector, including pharmacies
- Sensitizing policymakers on need for dedicated AYSRH programming and funding
- Advocacy to create a budget line for AYSRH
- Coach state team on scale up of best practices and train providers in AYFHS
TCI’s AYSRH approach scaled rapidly to 39 cities and multiple urban slums between 2018 and 2021 using its evidence-based interventions and coaching model. In the context of universal health coverage, TCI has supported segmented demand generation and improved access to quality and affordable contraceptive as well as youth-friendly health services. It provides a menu of interventions for cities to implement for youth – including such approaches as public-private partnerships with pharmacies and quality assurance using quick checklists – along with an innovative coaching model. The article concludes that TCI’s AYSRH approach has facilitated greater access to contraceptive methods of choice for youth.
* Just after the article was submitted, TCI added three additional AYSRH cities in the Philippines – bringing the total number of AYSRH-supported cities to 42.
Recent News




