
India Toolkit: Demand Generation
Enabling Urban Accredited Social Health Activists
 Purpose: This tool provides guidance on strengthening the role of urban Accredited Social Health Activists (ASHAs) through coaching and mentoring for facilitating utilization of quality Family Planning (FP) services among marginalized and vulnerable population in urban slums.
Purpose: This tool provides guidance on strengthening the role of urban Accredited Social Health Activists (ASHAs) through coaching and mentoring for facilitating utilization of quality Family Planning (FP) services among marginalized and vulnerable population in urban slums.
Audience:
-
General Manager FP
-
Urban and Community Process Manager
-
Joint Director/Additional Director
-
Chief Medical Officers (CMO)/Additional Chief Medical Officers (ACMO)
-
Divisional Urban Health Consultant (DUHC)/Nodal Officer-Urban Health and Family Planning/District Program Managers (DPM)
-
City Community Process Managers (CCPM)
-
Urban Health Coordinator (UHC)
-
FPLMIS Manager
-
Medical Officer In-charge (MOIC)
-
NGOs/Health Partners
Background:
ASHAs work as community level care providers. They play a vital role by facilitating communities’ access to health care services including FP with the aim to reduce preventable child and maternal deaths.
Urban ASHAs, as per the National Health Mission (NHM), work on the pattern of rural ASHAs and are the link between urban poor and public health services. The urban ASHAs visit household in their assigned catchment areas and spread awareness about range of health services including family planning. They also provide support to the Urban Health and Nutrition Day (UHND) sessions, organize and support monthly meeting of Mahila Arogya Samitis (MAS), which are community meetings for health awareness. (Refer to: Induction training module for ASHAs in urban areas – section 1, page nos. 7 to 13, for role of ASHAs).
Helpful Videos
Scope of ASHA’s Family Planning Work
- Maintain eligible couple’s household data in Urban Health Index Register (UHIR) or in similar registers.
- Devise FP due list from UHIR and prioritize non-users based on age/parity/method use for household visit plan.
- Provide information on FP basket of choice to help eligible couples in deciding and accessing the FP method of their choice, distribute oral contraceptive pills (OCPs) and condoms to those who wish to use them during their household visits.
- Undertake postpartum visits and counsel for FP
Evidence of Impact
Women/eligible couples contacted by ASHAs are more likely to be referred for family planning services.
TCI India technically supported government in coaching and mentoring of urban ASHAs through Lead-Assist-Observe (LAO) model and coached ASHAs on:
- Providing informed choice counseling and referrals
- Devising an “FP due list” of eligible couples based on UHIR and 2BY2 matrix data
- Using FP job aids and communication materials for counseling eligible couples and responding their questions about FP methods
- Linking the community with service delivery points
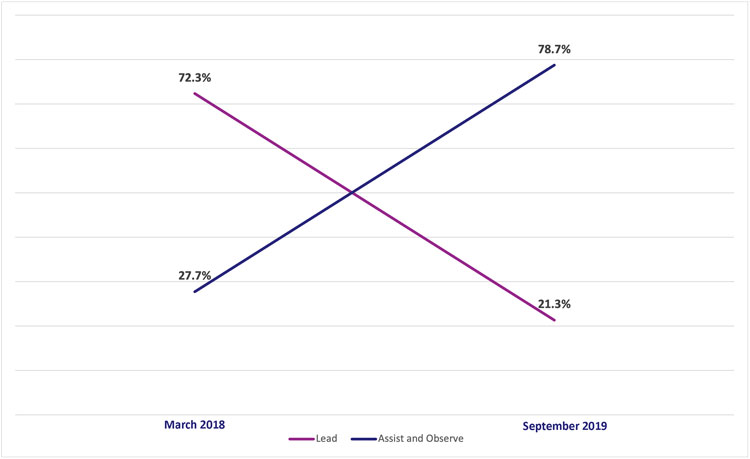
TCI India LAO coaching shows close to 80% ASHAs in Assist-Observe stage (Source : TCI India PMIS).
The PMIS data indicated that this strategy worked and increased skills and efficiencies of ASHAs to cater to the FP needs of the community. In Uttar Pradesh, over 20 months, around 6181 ASHAs were coached and over one million women were reached through the coaching calls. Around 80% of ASHAs shifted to ‘assist-observe’ stage from March 2018 (see graph below).
In addition, TCI India’s population based cross-sectional Output Tracking Survey (OTS) findings revealed that 28.7% respondents (currently married women between 15-49 years) had met ASHAs in the last 6 months. Around 27% respondents who were provided with information on FP visited any service delivery point (UPHC (11.9%), UHND (20.7%), Outreach camp (4.5%). Across all OTS cities, 51% of currently married women between 15-49 years and 36% of currently married women between 15-24 years were using a modern family planning method.
Guidance on enhancing the urban ASHA’s capacity as a family planning mobilizer
1. Onboard ASHAs and allocate the catchment area
Refer to the latest mapping and listing* data and ensure adequate numbers of ASHAs are on board as per population (1000-2500 population or 200-500 households per urban ASHA). After completing this step, define their catchment areas and coach them on the following areas mentioned below. In case adequate numbers of ASHAs are not on board to meet the requirement of the population, raise a request in the Program Implementation Plan (PIP) cycle or additional PIP cycle for the position of additional ASHAs. When the additional positions get filled then coach ASHAs as detailed below:
*Understand the role of urban ASHAs in mapping and listing of slum and population.
2. Identify FP and gender expert trainers:
Identify and hire trainers with extensive experience in FP to train ASHAs. During FP training, invite gender experts, male engagement programmers and gender champions (city and facility level) to facilitate a session on gender to orient and sensitize ASHAs so that they can integrate gender components into their FP activities.
(Refer to the List of master trainers to be sourced at the time of planning of training from states and ensure that trainer have gender perspective and sensitive towards issues.)
3. Specific and in-depth training of ASHAs on family planning
In general, when ASHAs are recruited they undergo initial training which include only one session on family planning. However, detailed and in¬depth training is required for them to provide quality information and services to the community. Thus, a two-day training, especially on family planning and informed choice counseling is necessary for ASHAs and this should include the following:
Update population register
Coach ASHA to map and list all households including the most vulnerable population (Refer to TCI India’s mapping & listing tool) and on updating her survey record or population register, specifically section-2 of UHIR (ASHA diary), termed as ‘slum/gram survey’ periodically. An updated survey reveals the total number of population to be served by an ASHA
In-Depth knowledge of modern contraceptive methods
ASHAs must be coached on the effectiveness, advantages, working mechanisms and side effects of each contraceptive They must be coached on providing informed choices to eligible couples, using FP job aids, promoting spousal communication and increasing male participation in family planning by supporting their spouse in FP decisions or by adopting a FP method. The training must integrate gender components, like use of gender-sensitive language, non-discriminatory practices in all interactions, addressing cultural and social norms that impact gender equality, use of simulation games on gender sensitization such as white and black marble game to change the mind-set of son preference, Kranti Bhranti an interactive game of Rashtriya Kishore Swasthya Karyakram (RKSK), and creating awareness on Pre-Conception and Pre-Natal Diagnostic Techniques (PCPNDT), etc. ASHA must also be coached on conducting Mahila Arogya Samitis (MAS) meetings.
Periodically a refresher training is to be conducted by MOICs on contraceptive methods by leveraging ASHA and ANM meeting platform.
Family planning job-aids
Each ASHA must be provided with FP job aids such as basket of choice, flyers on various FP methods, simulation games on gender on gender sensitization, flyers on various government schemes like Ensuring Spacing at Birth (ESB) and frequently asked questions with answers related to FP methods. Ensure FP job aids content should be gender sensitive. This will help ASHAs to provide more effective FP interpersonal counseling and create gender awareness during home visits.
Develop a due-list of eligible couples
Once the ASHA updates her UHIR, she then updates/completes section 9 of the UHIR, which is an aggregation of all eligible couples in the community. From this section, the ASHA can extract the eligible couples in the population she serves. Further, segregation of lists of eligible women based on age and user/non-user helps frame a duelist for counseling. Coach ASHA on the 2BY2 matrix tool developed by TCI India which helps them to segregate and prioritize eligible FP clients list based on parity and age (Refer to 2BY2 matrix tool).
Prioritize visits to eligible clients and integration into routine contact plan
When an ASHA extracts the due list from her UHIR, it gives her a clear picture of potential couples who are in high need of FP services. ASHA can take support of community health workers such as MAS and Anganwadi workers by sharing the duelist with them for better coordination. ASHAs precedence to this list during household visits. Also, the list is categorized into users and non-users; the ASHA is encouraged to devise a plan with her supervisor to meet non-users first and refer them to Fixed day static service (FDS)/Antral diwas, Khushhal Privar diwas, UHND and outreach camps. As for users, she must provide continuation support including both reassurance couple counseling to promote shared decision-making and support for contraceptive use In addition to that she also resupply of commodities such as condoms, Chhaya, and OCPs.
Training on Family Planning Logistic Management Information System (FPLMIS)
To strengthen supply chain and door step delivery of FP commodities Government of India (GoI) has devised a FPLMIS mobile software. The FPLMIS Manager must map the names of the current ASHAs and ensure their correct details are added at the backend of FPLMIS software. Every six months’ update FPLMIS portal by deleting the names of ASHAs who left job and adding the names of new ASHAs. The FPLMIS manager must coach both ANMs and ASHAs on the online indenting process and reorient them at least once every year. A poster/flex describing indenting process pictorially can be placed at each UPHC for easy reference.
Orientation on the benefits of government schemes related to their work
The FP incentive and ESB are government schemes to promote family planning and spacing between births. It is important that an ASHA feels motivated to work for FP. Hence, it is important to coach ASHA on the schemes, specifically on how to fill out the forms, when to claim, what are the criteria on which the incentives are given and where these should be submitted (Refer FP incentive and ASHA incentive scheme (Form 1 for payment of incentive amount to urban ASHA).
Family planning information dissemination and follow-up
ASHA must provide information and counseling on FP to motivate new users, and encourage regular usage and switching of methods, if necessary (Refer to Training module on Inter-Personal Communication; and method-specific training PPTs). During the home visits, Arogya Mela, Saas Bahu Beta Sammelan (SBBS), and UHND platforms, ASHA must conduct couple counselling, and encourage inter-spousal communication. ASHA should also encourage male partners to promote shared decision-making and support contraceptive use. ASHAs must identifying FP and gender champions from different NGOs, community, facilities and male engagement programs to build enabling environment. With the support of them, during SBBS and MAS meetings street plays (Nukkad Natak) can be used as a medium to spread the messages on FP and gender across community.
To ensure retention of the adopted method by the client, ASHAs must follow up with clients in the proposed interval and track the continuation of the FP method and track drop-outs. They should discuss with contraceptive users how the method has worked as well as any issues or difficulties that might have come up. ASHAs to ensure referral for management of any side-effect or complications.
Preparedness for emergencies
UHC/CCPM, MOICs should coach ASHAs on inclusion of FP under essential services and that they should regularly provide FP information and supplies during any emergency like the COVID-19 pandemic.
4. Coach ASHA supervisor Auxiliary Nurse Midwife (ANM) on mentoring and supporting ASHAs
Continuous on-the-job mentoring and supervision is required to help the ASHA translate her training into practice. Guidance on mentoring and supervision of ASHAs is provided in the handbook for ASHA facilitators, and includes a field-visit-checklist for supervisor and a checklist for feedback (Refer to : Guidelines for ASHA facilitators). Community Process Manager at the state level should be oriented on coaching CCPM on establishing the importance of building the capacities of urban ASHAs and ANMs on family planning. ANMs must be coached on the following:
- Providing handhold support to their ASHAs by initially accompanying them during a few household visits and later when ASHA face any challenges like counseling gatekeepers and decision-makers of the family. Review the eligible couple list and support in identifying non-users in the catchment area of ASHAs.
- Demonstrate the use of job aid and providing informed choice.
- Coaching ASHAs on availing benefits of the government schemes like ESB scheme and support in documentation
- Work related to UHIR, vouchers, ANMs can deploy a tactic of pairing up one good performing ASHA with other ASHAs to coach them on reports and voucher filling, completing and updating UHIR.
ANMs must take all the above steps when a new ASHA joins.
5. Establish ASHA and ANM meetings as a coaching mentoring platform
ASHA and ANM meeting platform lead by MOICs should be used to review, motivate and regularly coach ASHAs and ANMs, check UHIR and documentation work, and support low performing ASHAs. ASHAs should be encouraged to share positive experiences and challenges during ASHA and ANM review meetings. UHC/CCPM should also participate in ASHA and ANM meeting.
6. Recognize and reward performance
Recognizing and rewarding ASHAs who perform well, contributes to maintaining motivation of ASHAs and helps prevent drop-outs.
Roles and Responsibilities
Role |
Responsibility |
General Manager FP/Urban/Community Process Manager |
|
Joint Director/ Additional Director |
|
Chief Medical Officer (CMO)/Additional Chief Medical Officer (ACMO) |
|
Divisional Urban Health Consultant/Nodal officer-urban health and FP/DPM |
|
City community process manager/Urban Health Coordinator |
|
FPLMIS Manager |
|
Medical Officer in-Charge |
|
ANM (ASHA facilitator) |
|
NGO/Health Partner |
|
Monitoring of Performance and Outcomes
CMO, Nodal officer Urban and FP, CCPM and UHC monitor the ASHAs on a set of indicators, including ones based on the key tasks undertaken by them. These indicators can be obtained from the data in the HMIS, ASHA registers, ASHA facilitator reports and other activity reports, and include the following:
Number of:
- ASHAs deployed as compared to the numbers sanctioned
- ASHA and ANM meetings held as compared to those planned
- New family planning users enlisted by ASHA
- ASHAs trained compared to those deployed
- Eligible couples who received services from ASHA
- ASHAs who received supplementary training on family planning
- Post-partum and post-abortion family planning service users
Percentage of:
- ASHAs receiving supportive supervision from ANMs
- Post-partum and post-abortion family planning service users
- ASHAs who have stocks of both condoms and pills
- ASHAs who have made a prioritization plan for household visits to eligible couples and pregnant women
Additionally, it is important to monitor ASHAs through field visits, whether they have been provided job-aids and IEC materials and whether they are distributing IEC material to eligible couples. These indicators can be monitored during CMO meeting and UPHC level ASHA and ANM meetings. These meetings serve as a forum for sharing and validating information related to the performance of ASHAs and for problem solving.
Cost Elements
For strengthening ASHAs’ capacity to facilitate and support FP, requires that the following heads are budgeted. If they are not budgeted, then a request should be made in the Supplementary PIP and in the next year’s PIP (Refer to: TCI India’s PIP tool). The given table is indicative and illustrates the manner in which cost elements are provided in a Government PIP. Hence, it guides audience on where to look for elements related to a particular task, such as strengthening the urban ASHAs.
| Cost Element | FMR Code |
| Training of trainers on FP for cascade training to ASHAs | 9.5.22.1 |
|
Supplementary training on FP for ASHAs |
U.3.1.2 & U.3.1.3 |
| Job-aids, IEC material | 11.6.1; 11.6.3; 11.6.4; 11.6.5; 11.6.6; 12.3.4 |
| Commodities and supplies | U.6.2.4.1 till U.6.2.4.3 |
| ASHA FP incentives | U.3.1.1.1 till U.3.1.1.3; 3.1.1.2.2 till 3.1.1.2.8 |
| Budget for ‘Reward and Recognition’ of ASHAs | 3.1.3.3 |
| Orientation/review of ASHAs (as applicable) on; New contraceptives, post-partum and post-abortion family planning, scheme for home delivery of contraceptives (HDC), ensuring spacing at birth (ESB), wherever applicable pregnancy testing kits (PTK) | 3.1.2.5 |
* Source: NHM PIP Guideline 2018-2019
Sustainability
Ensuring the capacity of urban ASHAs to provide quality FP information and services requires concerted efforts on the part of the CMO to ensure that the costs for hiring, training and supervision/ mentoring of ASHAs, ASHA and ANM meeting are included in the PIP. Reward and recognition of well-performing ASHAs can provide motivation for their continued good performance.
TCI APP USERS PLEASE NOTE
You will only receive CERTIFICATES by email – when earning a score above 80% – and will not be able to view or print a certifcate PDF from the TCI app.
Test Your Knowledge
Earn a Certificate

Available Resources
- Induction Training Module for ASHAs in Urban areas_English, Section 1, Page No. 7 to 13
- Induction Training Module for ASHAs in Urban Areas_Hindi
- Flow Chart for ASHA support mechanism
- Support mechanism for ASHA under NHM
- GoI family planning method-specific training presentations
- GoI method-specific counseling cards on family planning
- GoI frequently asked questions & answers on family planning
- Pregnancy screening checklist
- Family planning effectiveness chart
- Family planning films by GoI
- Guidelines for ASHA Facilitators District ASHA Resource Center-Gujarat, Annexure-I & Annexure- II, from page no. 8 to 10
- Urban Health Index Register (UHIR)/Eligible Couple Register/ RCH register
- Urban Health Index Register
- RKSK Kranti Bhranti -Interactive Game
- NHM PIP guideline for a particular financial year
- TCI India’s mapping & listing approach
- TCI India’s PIP approach
- ASHA incentive scheme
- Form 1 for payment of incentive amount to urban ASHA
- 2BY2 Matrix tool






