“I have 5 children and I had no clue on available FP methods for me such as what, where, how and cost. ASHA [local peer educator] was meeting me regularly and informed me about all the methods but my husband said that there must be some benefit for ASHA. Later on I realized that how important it is for my family to plan the number of children… This time my husband … thanked ASHA to help us in all these. We are happy and making others happy to help them to get an FP service. It has changed our life and particularly my life.” – Gulshan, Woman from a Poverty Cluster in Aligarh

Poverty clusters are small and often surrounded by wealthy sectors. Women residing in these poverty clusters represent the poorest segment of society. They are marginalized from every type of health service, especially from family planning (FP) services. Image Credits: UHI, 2014.
There is a large discrepancy between the number of slums registered on Uttar Pradesh’s governmental lists and those that actually exist. The same holds true for the population living in the slums—many more people live in the slums than are recognized by the government. Poverty clusters are informal groupings of families, ranging from one to sixty or seventy households and are often inhabited by illiterate migrants who lack social recognition and cannot vote. Women residing in these poverty clusters represent the poorest segment of society. They are marginalized from every type of health service, especially from family planning (FP) services, as health departments lack information about the existence and the needs of this population.
The Measurement, Learning & Evaluation (MLE) Project’s Baseline Survey Report for the Urban Health Initiative (UHI) in the cities of Agra, Aligarh, Allahabad, Gorakhpur, Moradabad and Varanasi indicated that use of modern contraceptive methods was very low in the lowest wealth quintile – as low as 25.7% in the city of Aligarh. At the same time, the total fertility rate was highest for the poorest wealth quintile in the cities surveyed, between 4.0 children per woman in Gorakhpur and 5.3 children per woman in Aligarh.
Identifying the Unregistered Poverty Clusters

Poverty is a defining factor of both registered and unregistered slums in India’s urban areas. Image Credits: UHI, 2014.
In order to reach the poorest and most vulnerable populations with family planning (FP) information and services, UHI, with support from local partners, undertook a mapping exercise to identify unregistered slums and poverty clusters. UHI convened existing NGOs, Anganwadi workers (AWWs) and representatives of the World Health Organization’s and UNICEF’s polio program to discuss the clusters’ location and population estimates. Together they prepared a detailed list of poverty clusters that indicated the expected location and any relevant landmarks. The UHI team, with their NGO partners, visited each cluster to physically verify their existence and to determine the vulnerability of the inhabitants.
Once the clusters have been identified, peer educators and urban accredited social health activists (ASHAs) are deployed and conduct home visits, counseling sessions, group meetings and interactive events for cluster households. ASHAs have helped the women living in the clusters gain confidence to go to the hospital and adopt different contraceptive methods, such as sterilization or the insertion of an intrauterine contraceptive device (IUCD).

Women and children are especially vulnerable in poverty clusters. Image Credits: UHI, 2014.
UHI’s client outreach strategy, which focuses on using interpersonal communication through community-based resources, such as peer educators, to increase awareness and use of FP, has helped UHI connect with individuals in these poverty clusters. As a part of UHI’s Doctor at Doorstep Initiative, doctors and counselors visit poverty clusters to build community confidence and address any myths surrounding FP methods. UHI also conducts Community Health Days where services are directly available in the poverty cluster. Handouts with lists of FP methods with their prices and FP facility and/or with talking points for women to engage their family members of husbands about FP methods are distributed.
Other strategies, such as advocacy and expanded service delivery, have ensured that UHI has made the proper linkage between these underserved and vulnerable communities and FP service delivery points. UHI strategies and interventions are aligned with Government of India and Government of Uttar Pradesh strategies. UHI works very closely with the government at all levels (community, city, state and national level). UHI is a part of several task forces and technical support groups, advocating for (FP) and urban health.

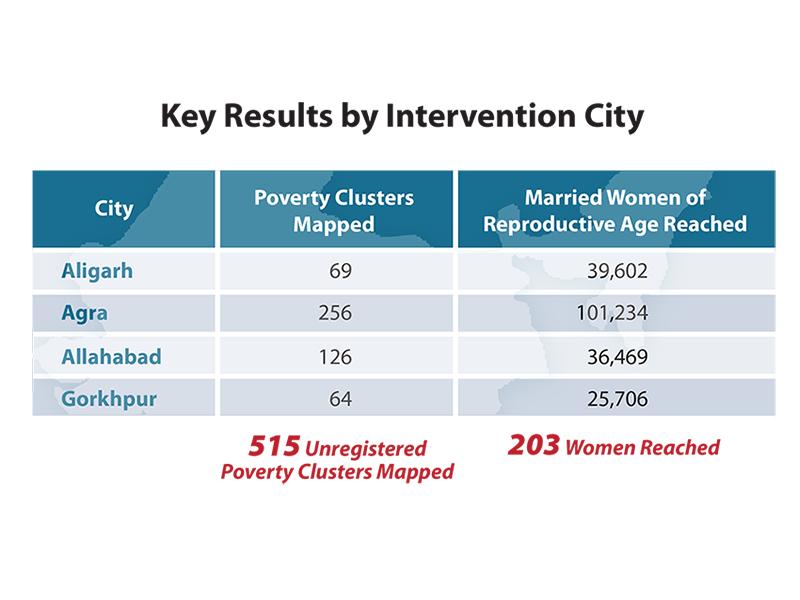
Overall, 515 unregistered slums and poverty clusters have been mapped in the cities of Agra, Aligarh, Allahabad and Gorakhpur. Over 203,000 married women of reproductive health were reached with FP messages through different activities promoted by UHI.
The program has also contributed to more women having access to and using contraceptive methods.
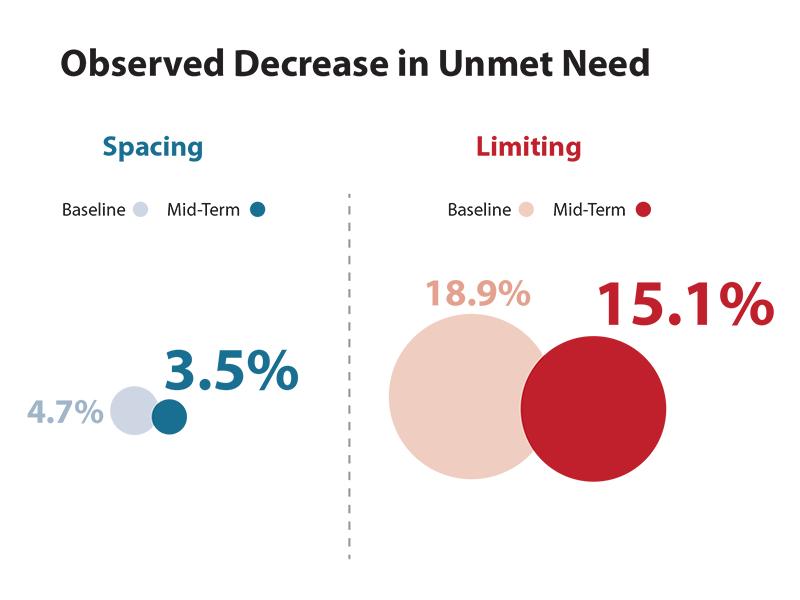
Based on data from MLE’s UHI mid-term evaluation, the percent of unmet need for FP has decreased since the start of the program (from a total of 23.6% and baseline to 18.6% at mid-term).
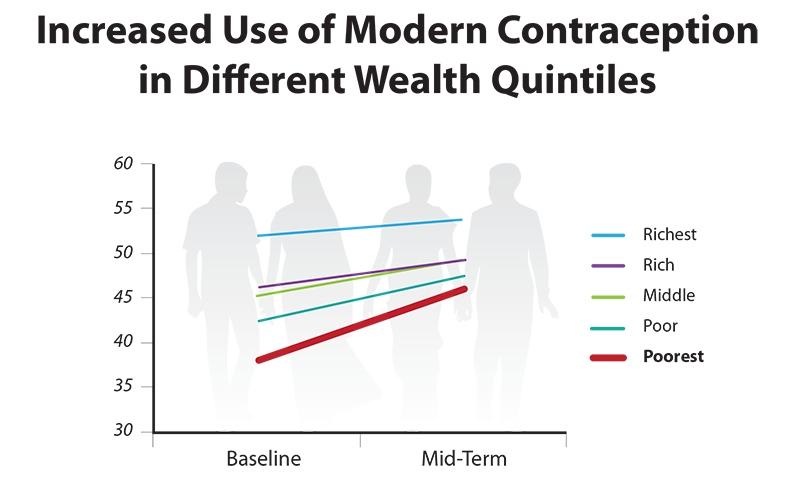
Use of modern contraception by women has increased from an average of 38.1% at baseline to 45.85% at mid-term.
“I used to see the women living nearby road in very temporary settlement and in small patches. I contacted my organization and mentioned that this population is not covered and in very vulnerable situation… It was very difficult to get the community rapport as they are most vulnerable women and are far away from health services as well as other basic needs. Slowly I got recognition among them and they started talking with me regarding health issues…They say me “you are our doctor” and it gives me real pay for my work. They consider me as their family member and of course they are my family.” –Seema Devi, Peer Educator (Urban ASHA) in Aligarh
This story was originally written by the Measurement, Learning & Evaluation Project, which evaluated the Urban Reproductive Health Initiatives (UHRIs) in Kenya, Senegal, Nigeria and India. The Challenge Initiative is charged with expanding access to the proven solutions and successes developed under the UHRIs.
