
India Toolkit: AYSRH Demand Generation
Priority Strategies for Improving Contraceptive Use Among First-Time Parents
 Purpose: This tool is an approach to reach first-time parents (FTPs) through frontline health workers or Urban Accredited Social Health Activists (ASHAs) to increase correct knowledge on modern contraceptive methods and improve contraceptive use among them.
Purpose: This tool is an approach to reach first-time parents (FTPs) through frontline health workers or Urban Accredited Social Health Activists (ASHAs) to increase correct knowledge on modern contraceptive methods and improve contraceptive use among them.
Audience:
- Additional Director/Joint Director/Divisional Program Manager
- Chief Medical and Health Officers (CMHO/CDMO/CMO)
- Chief Medical Superintendents (CMS)
- Divisional Urban Health Consultant
- Nodal Officer-Urban Health, Family Planning, Rashtriya Kishor Swasthya Karyakram (RKSK)
- Urban Health Coordinator/Assistant Program Manager, NUHM
- Medical Officer In-Charge
Background: The National Family Planning Health Survey (NFHS 4, 15-16) provides a growing body of evidence that the age group with the lowest contraceptive prevalence rate are married women between 15-29 years of age, more specifically young married first-time parents. This age group of 15-29 years face a unique set of challenges different to those faced by older married women with regards to accessing and availing family planning services.
Evidence of Impact
The Challenge Initiative for Healthy Cities (TCIHC) experience from five cities (Firozabad, Varanasi, Gorakhpur, Allahabad, and Saharanpur) revealed that when ASHAs are coached and mentored to periodically update urban health index register (UHIR), segregate and list women based on age and parity, they are able to prioritize young and low parity women, specifically first time parents for family planning. This practice also aids to maintain a registry of young married first-time parents (FTPs) 15-24 years, and prioritize the category for household visits. The coaching enables them to easily identify FTPs with an unmet need for FP methods and counsel them to avail family planning services on FDS days/Antaral diwas.
The strategy is showing promise as data from a population level survey among FTPs from the five AYSRH intervention cities indicate a 17% increase in modern contraceptive prevalence rate (mCPR).
Figure 1: Findings from two-rounds of Population based survey conducted by TCIHC
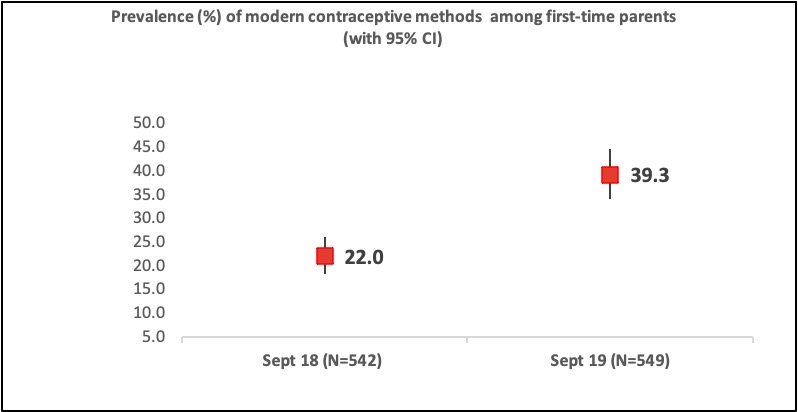
[1] TCIHC conducted two rounds of population based output tracking survey between September 2018 and September 2019.
Guidance on Scaling Up This Intervention
The following steps can facilitate a successful scale up of FTP interventions in a state:
Making FTP data visible
To amplify how health systems must focus and prioritize this group, data from population level studies, HMIS and project health information systems must be triangulated and discussed at both city and state level family planning monitoring meetings. Family planning uptake data disaggregated by age/parity and method choice is critical for a city to plan its strategy to reach women with unmet need for family planning. Making FTP data visible in city level monitoring meetings such as family planning review meeting/NUHM review meeting is therefore important.
Coaching & mentoring ASHAs
Coaching and mentoring ASHAs is an important step towards elevation / visibility of young first-time parents, so that FTPs are seen and served at UPHCs with the right, appropriate service including contraceptive methods.
ASHAs must to be coached to:
- Update population register: The importance of updating her survey record or population register, specifically section-2 of UHIR (ASHA diary), termed as ‘slum/gram survey’ periodically. An updated survey reveals the total number of population to be served by an ASHA.
- Develop a priority list of FTPs: Once the ASHA updates her UHIR, she then updates/completes section 8 of the UHIR, which is an aggregation of all eligible couples in the community. From this section, the ASHA can extract number of FTPs in the population she serves. Further, segregation of lists of FTP women based on age and user/non-user, helps frame a priority list of young first-time non-user parents for counseling.
- Prioritize visit to FTP (listing of FTP and integration in routine contact plan): When an ASHA extracts FTP list from her existing eligible couple (EC) section of the UHIR, it gives her a clear picture of potential women who are in high need of contraception for spacing between children. The list is shared with Anganwadi workers for better coordination. ASHAs precedence to this list during household visits. Also, the list is categorized into users and non-users; the ASHA is encouraged to devise a plan with her supervisor to meet non-users first and refer them to FDS. As for users, she provides continuation support including both reassurance counseling, and also resupply of commodities such as condom and pills.
- Leverage benefits of government schemes related to their work: ESB is a government scheme to promote spacing between births. It is important that an ASHA feels motivated to work for FP for first-time parents. Hence it is important to coach ASHA on this scheme, specifically on how to fill the form, when to claim, what are the criteria on which this incentive is given and where it is to be deposited (Refer to ESB scheme).
- Follow up: To ensure retention of the adopted method by the client, ASHAs must follow up with clients in the proposed interval.
Sensitization of the influencers (i.e., family/community) on the benefits of family planning
In many communities, it is still a taboo for a 20-22-year-old woman to adopt a family planning method (Hall, Stephenson, Juvekar, 2008). Therefore, ASHA must sensitize both FTPs and key influencers on the benefits of contraception for a young mother (and child), and this could include:
- Counsel FTPs on one-on-one basis to explain the benefits of spacing. IEC material may be used, if available.
- Educate influencers of FTPs including mother-in-law, sister-in-law, husband and, peers on the benefits of contraception for a young mother.
- Conduct meeting of FTPs where non-users can seek inspiration from the users and where couples can interact and discuss family planning amongst themselves.
You hold such an important position in the family and it is your decisions that have helped your children make wise choices. Family planning is important for the health of your daughter-in-law and your grandchildren, as well as for the financial situation of your family. The best thing you can do is to make the right decision for your son’s family.” — Laxmi, an ASHA in Ramnagar, Firozabad sensitizing the mother-in-law of a young woman who did not want her daughter-in-law to adopt family planning.
Whole-site orientation
To mitigate provider bias if any caused by inadequate knowledge on methods or the latest medical guidelines about them, it is critical to conduct ‘whole-site orientation’ of all staff working at the UPHCs on specific needs for FTP and the importance of offering them all methods and support them to choose a method of their choice.
Designate a day for FDS marked for FTPs at UPHCs and link with routine FDS/FPD/Antral diwas (spacing day)
Fixed day static/Family planning day (FDS)/Antaral diwas (spacing day) approach assures quality family planning services at a pre-fixed time known to the community. To demonstrate demand for family planning among first-time parents, the Chief Medical Officer (CMO) may decide to designate one of the routine FDS day from the FDS calendar to be marked as special FDS for FTP. Following this ASHA mobilizes FTPs, announcing the day and timing specially reserved for them to avail family planning services at the nearest UPHC. To highlight the special day, facility staff may provision counseling corners, display IEC materials on FP and create a visual enhancement of the facility.
In facility readiness, it must be ensured that counseling services are offered in person to maintain confidentiality. As demand for services among this group improves, the special FDS cycle maybe discontinued and services can merge with regular weekly FDS.
Learn more about how to organize FDS.
Inaugurate FTP activity in a new city
In a new facility or a city where a ‘Special FDS for first-time parents’ if is being done for the first time then getting this inaugurated from the Chief Medical Officer (CMO) can garner attention from neighboring facilities, local media and boost the morale of that particular UPHC staff.
Roles and Responsibilities
Role |
Responsibility |
| Additional Director/Joint Director/Divisional Program Manager |
|
|
CMHO/CDMO/CMO
|
|
| CMS |
|
|
Nodal Officer-Urban Health and FP
|
|
| Medical Officer-In-Charge |
|
| ASHA, Mahila Arogya Samiti (MAS), NGO, Outreach Workers |
|
Monitoring Benchmarks
- Number of FTPs identified by ASHA
- Number of FTPs reached by ASHA
- Number of FDS for FTPs organized
- Contraceptive uptake by FTP in each of the facilities
- Number of WSOs organized
- Number of meetings organized to influence non-users by users
- Number of one-to-one meetings with FTPs to brief them about benefits of family planning methods
- Number of FTPs reached in routine FDS/Antral diwas days after withdrawal of special FTP FDS
Cost Elements
The elements required for ‘reaching FTPs and improving their contraceptive behavior’ are mentioned below along with their Program Implementation Plan (PIP) codes for easy reference. They may be covered under existing budget line items, but if not, they should be incorporated through the PIP in the next cycle. Besides, any additional support can also be sought from the flexi-pool.
| Cost elements/PIP budget head | FMR code |
| Demand generation, strengthening service delivery | 1.1.3.2.1; 3.2.1 |
| IEC, Mid Media, Mass Media | 11.6.1; 11.6.3; 11.6.4; 11.6.5; 11.6.6 |
| Inter personal communication | U.11.3; 11.6.2 |
| Necessary Kits, surgical equipment and supplies | U.6.1.1 & U.6.1.2; 6.1.1.3.a till 6.1.1.3.f |
| Printing of FP manuals, guidelines | 12.3.1 till 12.3.5 |
| Training & capacity building, additional manpower | U.8.1.8.1.2; U.9.5.1 till U.9.5.8; 3.1.2.5; 9.5.3.1; 9.5.3.1 till 9.9.3.27 |
| POL for family planning/others (including additional mobility support to surgeon’s team if required) | 2.2.1 |
| Drop-back scheme | 7.3 |
| Quality assurance | U.16.2.1; U 13.1.1 & U.13.2.1 |
Source: NHM PIP Guideline, 2018-19
Note – The table above is indicative and illustrates the manner in which cost elements are provided in a government PIP, thus giving guidance on where to look for elements related to a particular task.
Sustainability
Family planning demand among FTPs can be sustained by linking them regularly with routine FDS/Antral diwas after withdrawal of special FTP-FDS and ensuring all providers of the facility and community regularly provide family planning services to young FTPs. Moreover, the rising demand among FTPs for family planning services will sustain this approach.
TCI APP USERS PLEASE NOTE
You will only receive CERTIFICATES by email – when earning a score above 80% – and will not be able to view or print a certificate PDF from the TCI app.
Test Your Knowledge
Earn a Certificate
Government of India Resources
- Induction Training Module for ASHAs in Urban areas_English, Section 1, Page No. 7 to 13
- Induction Training Module for ASHAs in Urban Areas_Hindi
- Guidelines for ASHA Facilitators District ASHA Resource Center-Gujarat, Annexure-I & Annexure- II, from page no. 8 to 10
- Flow Chart for ASHA support mechanism
- Contraceptives Display Kit
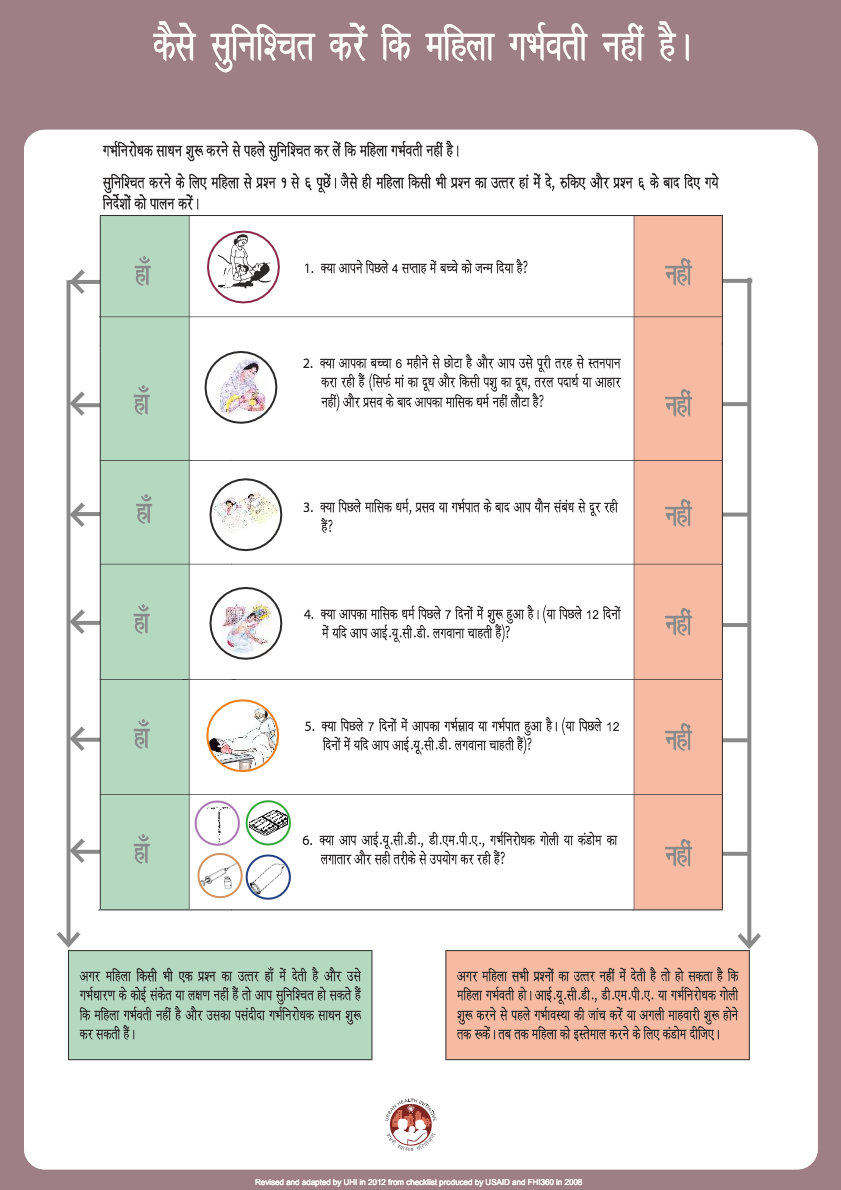
- Pregnancy screening checklist
- TG Segmentation Matrix
- Method Specific Training PPTs
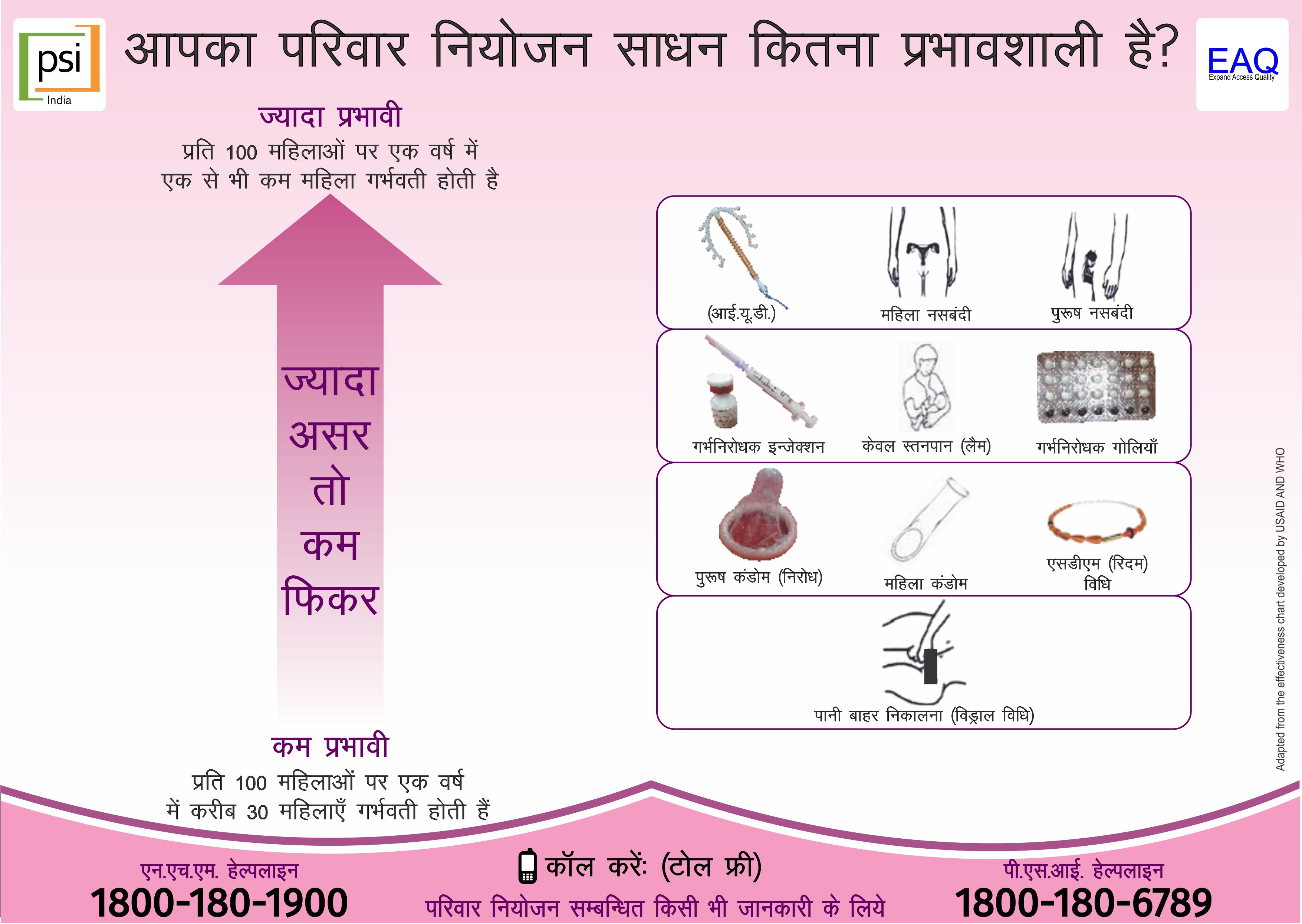
- Method Specific counseling cards/job aids
- Frequently Asked Questions and Answers
- Urban Health Index Register
- Facility Readiness Checklist
- Quality Assurance Parameters for Family Planning
- ASHA incentives scheme
External Resources





{kind=link}
{kind=link}
{kind=link}