
Pakistan: Service Delivery
Postpartum Family Planning
 According to the World Health Organization (WHO), postpartum family planning (PPFP) is defined as the prevention of unintended pregnancy and closely spaced pregnancies through the first 12 months following childbirth, but it can apply to an “extended” postpartum period up to two years following childbirth.
According to the World Health Organization (WHO), postpartum family planning (PPFP) is defined as the prevention of unintended pregnancy and closely spaced pregnancies through the first 12 months following childbirth, but it can apply to an “extended” postpartum period up to two years following childbirth.
PPFP services can opt-in the following timelines post-delivery:
- Immediately postpartum (IPPFP) – within 48 hours
- During early postpartum (EPPFP) – 48 hours up to 6 weeks
- Including extended postpartum (EPPFP) – 6 weeks to one year after delivery
What are the benefits of PPFP?
- A woman can be fertile again after two weeks postpartum. Although breastfeeding serves as a natural way of contraception, it is not a 100% safe method for contraception.
- Acquiring a PPFP service and birth spacing method benefits both the mother and baby to a greater extent. As the mother’s body and health rejuvenate postpartum, the baby, her family, and her household are also restored with time. The World Health Organization (WHO) recommends at least 24 to 33 months of birth spacing between each live birth for a healthy family and effective financial outcomes.
- Birth spacing allows the family to provide a better quality of life for the children, their education, upbringing, nutrition and overall wellbeing.
How to implement
Step 1: Determine which contact points will integrate PPFP based on country-level data
According to the Population Demographics Health Survey 2018 (PDHS) report, Pakistan’s total fertility rate (TFR) is 3.8. On average, a Pakistani married woman of reproductive age (MWRA) carries three children in her lifetime, and every 1 in 4 does not make it because of malnutrition. Here we also need to focus on the fact that only 29% of women use PPFP at six months postpartum, whereas only 9% use family planning one month postpartum.
In this situation, family planning professionals and government officials need to develop a central ecosystem to provide PPFP services to mothers postpartum. You can leverage both public and private hospitals, rural health centers, Basic Health Units (BHUs), Community Health Workers (CHWs), Lady Health Workers (LHWs), Lady Health Visitors (LHVs), Community Midwives (CMWs), chemists, and male physicians to meet the need for short-term and long-term contraceptives.
Step 2: Prepare the facility by carrying out a facility assessment for the provision of PPFP
It is essential that you know all the healthcare centers providing maternal, newborn and child health (MNCH) services in your districts. Once you have determined step 1, you need to prepare the facilities by assessing the current status and availability of equipment. This assessment will also help you evaluate the service providers’ skills, knowledge and attitudes. Evidence suggests that a nicely equipped and well-ventilated clinic increases clients’ trust in the service providers. Ensure that the clinic has all the necessary commodities to address the client’s needs. The ideal situation would be that the labor room staff is equipped with the skills and equipment to provide immediate postpartum services. Moreover, counseling on PPFP should start at the time when women are coming for antenatal visits. Identified service areas also be assessed to see that they have the appropriate equipment, stationary, information, education, and communication (IEC) materials and job aids, commodities, and reporting tools. For example, providers working in the postpartum ward may need IEC materials on immediate postpartum IUD provision.
Step 3: Encourage informed choice and decision-making
Delineate the client on the least to most effective contraceptive methods to be informed and make an informed choice.
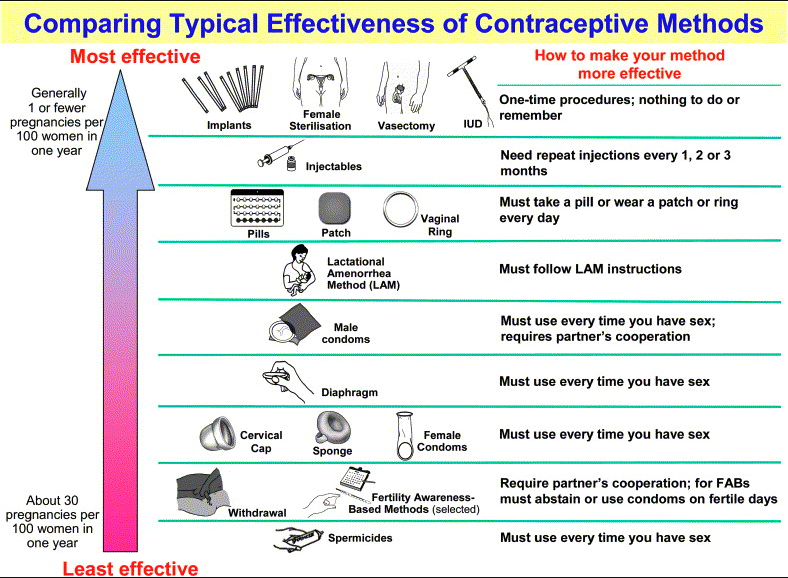
Source: WHO, 2006.
While counseling patients on what contraceptive methods would be beneficial, also explain to them the timing for FP services postpartum during their antenatal visits. WHO recommends that pregnant women have their first contact in the first 12 weeks’ gestation, with subsequent connections taking place at 20, 26, 30, 34, 36, 38, and 40 weeks gestation. However, you must accentuate at least four antenatal visits during pregnancy.
Recommended schedule for minimum required antenatal visits (WHO FANC Model):
| First (Booking) Visit | (Between 8-12 weeks) |
| Second Visit | (Between 24- 26 Weeks) |
| Third Visit | (At 32 Weeks) |
| Fourth Checkup | (Between 36-38 Week) |
| More Checkups | As advised by the Skilled Birth Attendant (SBA) |
Place pictorial IEC materials in local and regional languages to create awareness.
Here you also should assess the lactational status of the MWRA and suggest methods that are indicated for her to be able to make an informed choice. It is generally recommended that breastfeeding mothers should not use hormonal methods of contraception that contain estrogen (e.g: combined oral contraceptives, the vaginal contraceptive ring, and the contraceptive patch).
Step 4: Train providers on PPFP and PPIUD
Service providers should be trained according to the country’s national guidelines on family planning (both PPFP and PPIUD), usually developed by the Ministry of Health. While Step 1 will be the cornerstone for this approach, you should provide the necessary training to engage the health care providers.
Examples of Training Materials
- Guidelines on Birth Spacing and Family Planning for Midwives in Pakistan (Urdu)
- Standardized Training Package on Family Planning, WHO 2020 (Urdu) (English)
- Guidebook for Trainers on Healthy Timing and Spacing of Pregnancies (Urdu)
- Standardized Training Manual of Family Planning for CHWs, WHO 2020 (Urdu)
- Providing Post Pregnancy Family Planning Clinical Services, UNFPA & Jhpiego 2021 (English)
- Post Partum Family Planning Contraceptive Technology Update: Trainer’s Manual, Jhpiego 2012: Strengthening Post Partum Family Planning in Punjab (English)
- Post Abortion Family Planning Trainee Manual, Marie Stopes Society 2013 (English)
- National RMNCAH&N Strategy 2016-2020
Step 5: Engage in social mobilization activities to identify pregnant MWRAs in the community
Door-to-door activities can support the uptake of PPFP services in communities where CHWs can be deployed to generate demand for birth spacing and informed choice, especially among first-time pregnant women. CHWs can further identify homes where any woman is pregnant and create a referral for her to manage antenatal care. CHWs can do follow-up visits in such houses to complete the treatment loop.
Step 6: Document PPFP uptake
Ensure that service providers record the data and timeline of any woman coming in for a PPFP service to contribute to the national data.
Step 7: Conduct monthly review meetings to monitor progress
A monthly review meeting looking at the data on immediate PPFP will help to strengthen the quality of services.
Indicators for success
- Increase in clientele
- Increase in revenue
- Number of MWRAs reached/counseled
- Number of MWRAs registered
- Number of tokens generated/referrals provided
- Number of tokens redeemed/referrals completed
- Number of short-term contraceptives (condoms, pills, and injectables) purchased/distributed
- Number of IUCDs inserted (long-term contraceptive)
Resources needed
- Infrastructure (material to upgrade clinics)
- Printing costs for IEC material, brochures, client record books, client registration, and referral books
- Venue for training
- Logistics (transport, per diems, lunch)
- Accommodation (depends on the number of training days)
What Is the Evidence?
- Greenstar’s Social Marketing Program strengthened PPFP in six districts of Pakistan. In three years of program execution, we generated almost 39,000 PPFP clients, of which 10,000 were married between the ages of 15 and 25 years old. The program used social franchising, social marketing, and social mobilisation model to advocate for PPFP and its benefits in the communities via 576 Sitara Bajis (SB)–Greenstar’s trained social mobilizers–tagged with 610 service providers. After the program, around 80 SBs were rehired by the service providers to generate demand and create referrals to their clinics.
- 95% of women who are 0–12 months postpartum want to avoid a pregnancy in the next 24 months, but 70% of them are not using contraception (Ross & Winfrey 2001).
TCI APP USERS PLEASE NOTE
You will only receive CERTIFICATES by email – when earning a score above 80% – and will not be able to view or print a certifcate PDF from the TCI app.
Test Your Knowledge
Earn a Certificate

Tips
- During ANC counseling, health care providers should counsel clients on family planning options.
- Provide IEC materials on PFFP messages posted in maternity, labor and delivery, and gynecology wards.
- Ensure that the Department of Health’s family planning forms are available at all service delivery points and used.
- Consider holding dedicated PPFP days during the extended six weeks for immunization visits at health service facilities.
Challenges
- Lack of space or infrastructure may impact the ability to ensure privacy for clients and make it feasible to add family planning services.
- Additional initial costs are likely to be associated with integration (for example, the need for extra staff, training, IEC materials, and reporting tools).
- Providers may experience increased workloads.
- Clients may experience increased waiting times due to more extended, more comprehensive visits.
- Counselors without clinical training may be intimidated to discuss contraceptive methods and how they work.
- Documentation on whether or not FP counseling in antenatal care and delivery and adoption of method or referral back to health centers for follow-up care and management needs to be strengthened.
Related Resources
- High Impact Practices in Family Planning (HIP) Brief on Postabortion Family Planning
- HIP Brief on Family Planning and Immunization Integration
- USAID Global Health Learning Center course on Postpartum FP
- USAID Global health Learning Center course on FP and HIV Service Integration



