East Africa Toolkit: Services & Supply
Family Planning Integration
 This tool gives guidance on how to integrate family planning into other health service areas in order to reduce missed opportunities.
This tool gives guidance on how to integrate family planning into other health service areas in order to reduce missed opportunities.
The key areas for successful integration include, but are not limited to:
- Antenatal clinics
- Child welfare services
- Outpatient
- Maternity
- Comprehensive care unit
- Postnatal clinics
- Pharmacy
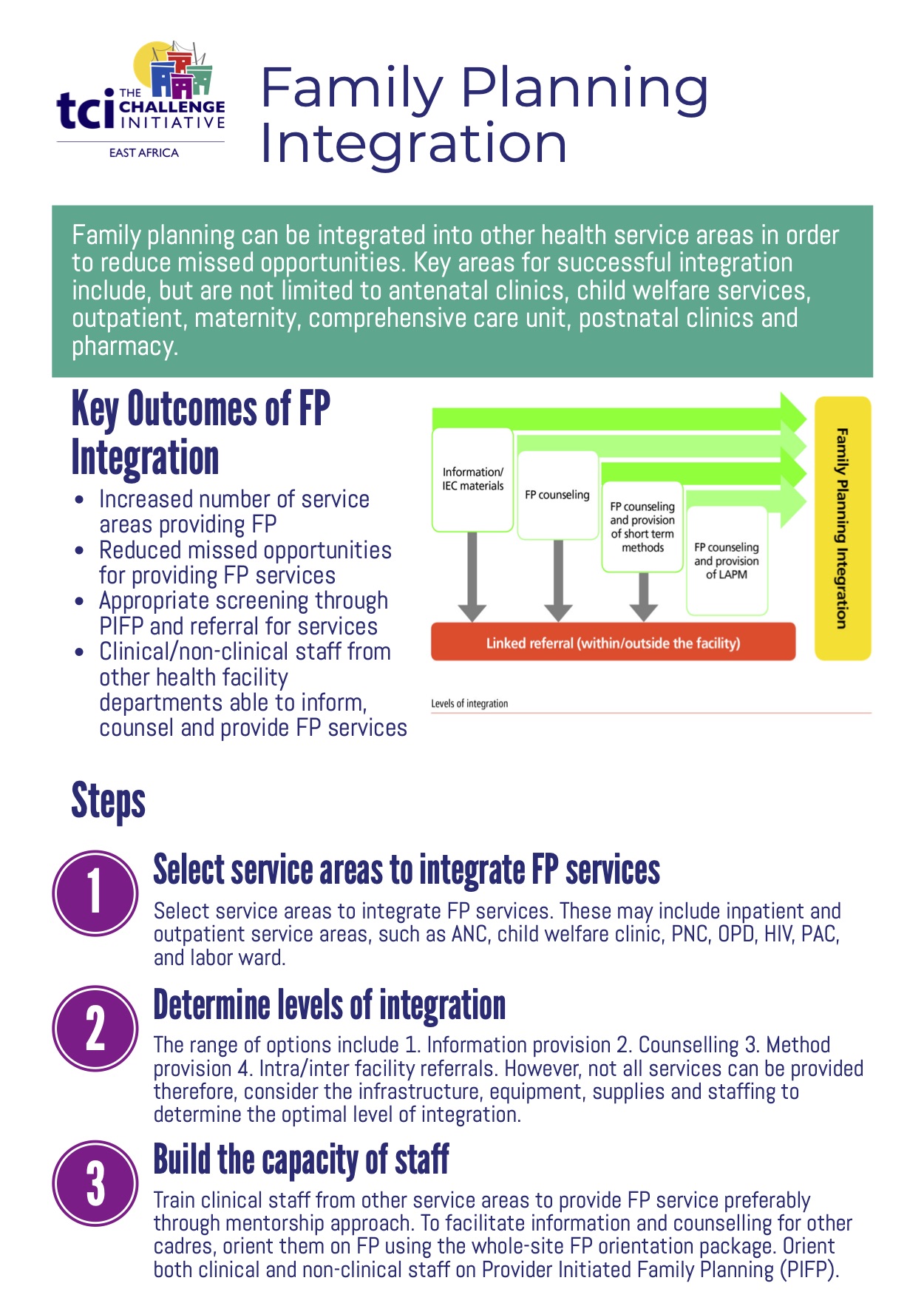
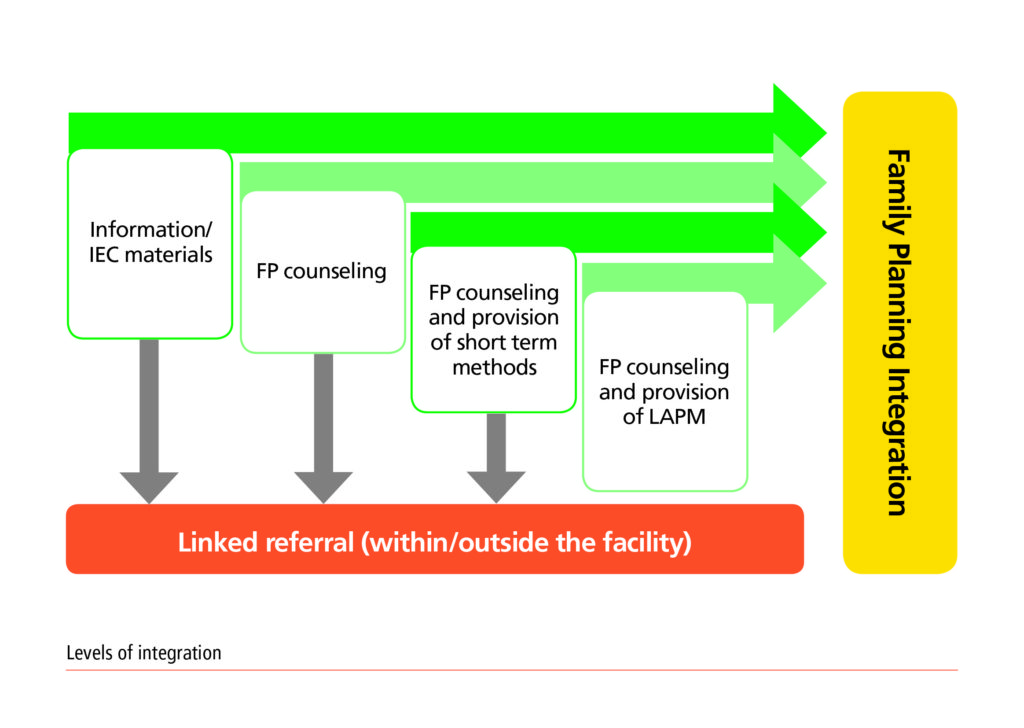
Integration Levels
Integration of family planning will be directed or agreed upon by the health facility. A facility implements a level within a service area dependent on staffing, availability of equipment and client flow, among others.
The diagram below highlights 4 levels of family planning integration.
Why Family Planning Integration Is Important
- Creates an opportunity to introduce family planning to new clients
- Increased number of service areas providing FP, leading to improved family planning service utilization at the facility level
- Addresses missed opportunities for accessing family planning for clients visiting a health facility for other services
- Tupange/MLE data on missed opportunity showed that 63% of women have missed an opportunity for family planning
- Clinical/non-clinical staff from other health facility departments able to inform, counsel and provide FP services, reducing unmet need
- Offers a one-stop shop where clients receive multiple services, reducing the number of facility visits
Evidence
- According to the Tupange FP Integration 2013, integration would take place in all service areas but at varying levels. HIV and postnatal wards had the highest levels of FP integration while child welfare clinics recorded the least level of integration
- Between 2012 and 2014, Tupange supported 55 facilities that reached about 6,259 new FP receptors
- Service areas have introduced integrated FP services other than in the FP room (96% of facilities were offering FP in at least 2 additional service areas). In the Tupange Project, the following results were achieved through integration of FP into other services:
- Over 40,000 clients were reached with family planning service between Aug 2012 and Apr 2014 through other service areas
- Over 19,000 clients were reached with family planning service over the same period through internal referrals from other service areas.
-
Testimonials: “Integration of FP services in Makadara Health Centre has been happening but at a small scale and with minimal documentation. The focus has been integrating HIV services to other service areas. With whole-site FP orientation, facility-based FP mentorship, better FP commodity management skills, most staff are now able to give FP information and/or services. This greatly reduces the missed opportunity for FP. Integration has made staff rotations easier” –Grace Mwakesi Facility, in charge of Makadara Health Center
Guidance: How to Integrate Family Planning Services
The following are some of the important steps to family planning integration:
- Carry out initial assessment and identification of facilities using agreed upon criteria. The criteria for selecting facilities should focus on institutions that have shown some level of preparedness and readiness in terms of space availability, equipment and staffing in delivering services, information and counseling
- Select service areas to integrate services map out available resources
- Important areas to consider for family planning services:
- Antenatal
- Child Welfare (immunization, sick/well baby clinic)
- Postnatal
- Outpatient clinical
- HIV services
- Inpatient clinical services:
- Labor ward
- Postnatal ward
-
- Information, Education & Communication (IEC) materials/family planning counseling
- Family planning counseling and provision of short term methods
- Family planning counseling and provision of long-acting and permanent methods (LAPMs)
- Family planning counseling and referral to the room for family planning services
- Determine levels of integration based on a 1-4 scale, where 1: information provision, 2: counseling, 3: method provision, 4: intra/inter-facility referrals. Not all services can be provided, so consider the infrastructure, equipment, supplies, and staffing to determine the optimal level of integration.
- Build the capacity of service providers. Technical service providers are expected to carry out family planning integration as per the national guidelines. Consider offering regular training and skills updates to help increase competence and confidence of the providers in delivering quality services.
- To facilitate information and counseling for other cadres, orient using the whole-site orientation package. Introduce Provider Initiated Family Planning (PIFP) to both clinical and non-clinical staff. This process is recommended to assist both the health provider and clients identify unmet needs for family planning.
- Equip the integration service areas with relevant equipment, stationary, IEC/job aids, FP commodities/supplies, referral tools and reporting tools. Needs will vary by integration level.
- Brand the service delivery areas to inform clients on availability of family planning services.
- Ensure documentation of all services provided (e.g. information, counseling, referral, and FP method) at the integration service area. Use existing tools such as FP registers. Consolidate and report the data from the integration area using existing reporting channels.
The following are some of the potential barriers to integration of family planning into other services:
- Infrastructure challenges, e.g., inadequate space to conduct additional services or client privacy
- Additional costs associated with integration such as extra staff, meeting training needs and extra IEC materials and reporting tools as required
- Increased workload in specific service areas and client waiting time
Tips
- Facilities that are more amenable to integration are those that have adequate space, equipment and staffing.
- Add integration service areas gradually after assessing the work load, data and supplies.
- Minimize the documentation requirements to keep the workload manageable.
- Label new integration service areas to increase awareness of FP services.
- Facilities should monitor integration services to ensure that client waiting time is not too long.
- Out of facility services should also be integrated with FP.
Monitoring Processes
- Monitor level of integration at the facility to assess progress/extent of integration. This should be guided by the facility family planning focal person
- Monitor facility service areas reporting integration through facility activity summary forms
- Monitor quality of family planning service delivery
Success Indicators
- Number of facilities offering integrated family planning services per service area
- Proportion of new family planning acceptors from integration points
Cost
- Training costs on skills update for service providers (stationery, training manuals, trainer’s fee, printing of certificates)
- Cost of materials for integration (IEC materials, job aids, data collection tools, referral booklets, summary books)
- Cost of family planning equipment, e.g., IUCD and implant sets
Sustainability
- Support and buy-in by the facility administration
- Inclusion of family integration as a regular part of health facility services
- Continuous Medical Education (CMEs) and mentorship to optimize the quality of service provision
- The local government support supervision team carries out quality audits on a regular basis. This include assessment of infrastructure, service delivery and human resources. Hold external and internal support supervision to ensure quality services. This could include:
- Quality improvement teams hold monthly meetings where quality is discussed and steps taken to maintain high standards of service delivery
- Linking it to the existing government strategy on integration (e.g., Community Strategy/Integration, etc.)
- Inclusion of family planning the government annual work plans, Costed Implementation plans
- Building capacity to critical mass
- Use of private sector-funded mechanism, e.g., Output Based Approaches (OBA) and franchise
TCI APP USERS PLEASE NOTE
You will only receive CERTIFICATES by email – when earning a score above 80% – and will not be able to view or print a certificate PDF from the TCI app.
Test Your Knowledge
Earn a Certificate