High-Impact Practice
Integrating trained, equipped and supported community health workers (CHWs) into the health system.
What Is It?
 Volunteers or paid employees that bring health information and services to people where they live and work, rather than requiring clients to visit a facility. Community health workers (CHWs) are an important cadre of workers in a health system. Personal contact with such a well-informed community member can help alleviate women’s and men’s fears about family planning, present contraceptive method options for spacing or limiting births, and facilitate access to family planning and other related services, such as maternal, neonatal and child health services, in both the government and private sector.
Volunteers or paid employees that bring health information and services to people where they live and work, rather than requiring clients to visit a facility. Community health workers (CHWs) are an important cadre of workers in a health system. Personal contact with such a well-informed community member can help alleviate women’s and men’s fears about family planning, present contraceptive method options for spacing or limiting births, and facilitate access to family planning and other related services, such as maternal, neonatal and child health services, in both the government and private sector.
Using CHWs is a globally recognized effective approach to increasing uptake of family planning. When trained and provided with the necessary tools and resources, CHWs can help fill gaps in both demand generation and service delivery.* These community-based activities can take place at the home, at work, or other spaces where people gather, such as marketplaces, mosques or churches, and community meetings and celebrations.
*Most CHWs are allowed to provide non-clinical contraceptive methods – condoms, pills, fertility awareness methods.Many countries also allow CHWs to give injectable contraceptives, and some are even moving toward allowing them to give implants.You should check with your country’s family planning service delivery guidelines to see who is allowed to provide different methods.
What Are the Benefits?
- CHWs are trusted community members with the knowledge and understanding of their communities’ unmet needs for health and family planning.
- They are often recognized and mandated by the Ministry of Health to provide health services.
- CHWs can contribute to reduced waiting times at facilities if a woman can get her preferred method from a CHW (usually pills or condoms, and sometimes injectables or implants).
- Task sharing selected family planning interventions to CHWs, such as counseling, can relieve the workload of higher-level providers, allowing them to focus on quality provision of provider-dependent methods such as the intrauterine device (IUD) or sterilization.
- When linked to health facilities, CHWs can refer clients for contraceptive methods that they themselves cannot provide.
- CHWs can provide follow-up care, for example, home visits after delivery.
How to Implement?
The decision to use CHWs and a community outreach strategy should not be taken lightly. While extremely effective, it is a major undertaking that takes careful planning, initial and refresher trainings to keep CHWs’ knowledge and skills up to date, ongoing supervision that is supportive and effective, and continuous monitoring for adjustments.
The following are general guidelines for TCI geographies to follow, but understand that there are many models for using CHWs in family planning that have been found to be successful.
Identify Existing CHWs Who Can Provide Family Planning Information and Services
Working with existing CHWs also relieves the burden of recruiting and selecting new CHWs, which can take considerable time and thought. New CHWs may also need approval by the government, another time-intensive process.
Finally, CHWs are likely already linked to a health facility, a national or regional health worker program, or an NGO. You can partner with these institutions to enhance your program as well as draw upon their resources and technical expertise.
Assess the CHWs’ Level of Education, Capacities and Resources
- What is the highest level of education they have attained? Are they literate?
- What training have they received?
- Who is supervising them? To whom do they report?
- Who else is on their health team (if there is one)?
- What tasks are they already expected to carry out?
- Are they expected to keep records and follow up with clients/community members?
- Are they paid or unpaid/volunteers?
- If volunteers, what motivates them to do their work?
- Do they have resources to travel? From whom do they get the resources?
This resource from the Maternal and Child Health Integrated Program describes comprehensively the considerations program planners need to make when determining the roles and tasks of CHWs.
Determine What Responsibilities to Give CHWs
CHWs can take on a variety of family planning responsibilities depending on their level of education and training. After considering the answers to the questions posed in Step 2, you should decide whether CHWs will:
- Provide contraceptive methods in addition to counseling, and if so, which methods
- Provide counseling only, and referrals for provision of methods
- Conduct awareness-raising activities around family planning and its benefits
These decisions may depend on your country’s laws and policies.
Train the CHWs
Your national Ministry of Health will likely have training materials for CHWs based on your country’s laws and policies. If not, the following globally accepted guidelines and materials can be adapted for your context.
 The Training Resource Package for Family Planning, a comprehensive website supported by the World Health Organization (WHO), the United Nations Population Fund (UNFPA), and the United States Agency for International Development (USAID), offers curriculum components and tools for trainers to design, implement, and evaluate family planning and reproductive health training workshops. All materials can be downloaded for free, and you may adapt or translate them for your own work.
The Training Resource Package for Family Planning, a comprehensive website supported by the World Health Organization (WHO), the United Nations Population Fund (UNFPA), and the United States Agency for International Development (USAID), offers curriculum components and tools for trainers to design, implement, and evaluate family planning and reproductive health training workshops. All materials can be downloaded for free, and you may adapt or translate them for your own work.
 K4Health Toolkits are practical collections of trusted global health resources, chosen by experts and arranged for easy use. They include a number of toolkits related to contraceptive methods, including pills, condoms, injectables, implants, the IUD, and permanent methods. The Toolkits include links to resources in multiple languages and country-specific information when available.
K4Health Toolkits are practical collections of trusted global health resources, chosen by experts and arranged for easy use. They include a number of toolkits related to contraceptive methods, including pills, condoms, injectables, implants, the IUD, and permanent methods. The Toolkits include links to resources in multiple languages and country-specific information when available.
 The Global Health eLearning Center, supported by USAID, provides many self-paced Internet-based courses that are easily accessible to the entire international health community. Some courses are in French. We recommend starting with the courses under the Family Planning Methods and Family Planning Programming topics.
The Global Health eLearning Center, supported by USAID, provides many self-paced Internet-based courses that are easily accessible to the entire international health community. Some courses are in French. We recommend starting with the courses under the Family Planning Methods and Family Planning Programming topics.
To learn how Tupange Pamoja developed a CHW program that followed national guidelines and also served program needs, see the East Africa Toolkit.
Most countries require CHWs to be linked to a specific health facility or post as part of the community health system structure to ensure the necessary supervisory structures, supply chain logistics and referral relationships are in place.
Your program can build on this by providing resources to strengthen the linkages, such as supervisory tools or referral cards. CHWs linked with a facility can help with the facility’s mobilization activities, to publicize the services that are available and ensure a steady stream of clients for the facility to serve.
- CHWs may be the only link that a community member has with the facility.
- Referrals of clients from CHWs can be strengthened if facility providers recognize and appreciate the work of the CHWs.
- CHWs can perform outreach to community members and mobilize them for facility-based services.
Provide CHWs with Adequate Equipment and Supplies
Offer Supportive Supervision
Make sure CHWs are operating within a system that will support and guide them in their responsibilities. For example, supervisors should routinely oversee the activities of the CHWs and hold monthly meetings to provide feedback. Monthly meetings can also serve as a way to provide family planning updates to CHWs and discuss myths and misconceptions encountered in the community. Periodic group meetings where all CHWs in a specific area attend can serve as a forum for CHWs to discuss common challenges and brainstorm solutions as a group. They can also be used to recognize high-performing CHWs and distribute certificates. TCI coaches local governments to complete a monthly performance evaluation form during supportive supervision visits with CHWs, which you can adapt for your context.
Consider Using CHWs Creatively for Demand Generation Activities
CHWs can be trained to be facilitators of discussion groups among community members to further reinforce family planning information received from radio programs, TV dramas, theater performances, and other communication materials. CHWs can raise additional issues, answer questions and further educate community members in a safe space. For example, TCI developed a Facilitator’s Guide Training Community Leaders, Champions and Gatekeepers on Family Planning to be used as part of community dialogues.
CHWs can serve as mobilizers for community health service days.
- In East Africa and Nigeria, prior to in-reaches, CHWs and social mobilizers conduct publicity and promotional activities for the service day so that community members who want long-acting reversible contraceptives (LARCs) can plan for it.
- In Francophone West Africa and India, on special family planning service days (en français) and fixed day static service, community relays and ASHAs help to raise awareness of the date and location of the free family planning service and of the methods that would be available. They also provide initial counseling and information on the various methods available.
- ASHAs in India are also critical for the successful implementation of adolescent health days and male engagement strategies,
CHWs can make personal visits to homes or to workplaces.
- In India and Francophone West Africa, ASHA and community relays make house-to-house visits to sensitize people on the benefits of family planning and provide accurate information on the methods available at their nearest clinic. Using interpersonal communication skills, these frontline health workers talk to women, husbands, mothers-in-law, youth and adolescents, and religious and community leaders to dispel any incorrect information and myths about family planning. In Francophone West Africa, the community relays use a modified version of a provider-initiated family planning tool to identify women with unmet need for family planning and refer clients to the nearest health facility if women express a desire to use a modern method.
CHWs can help map urban slums to ensure these underserved areas are targeted by program activities.
- In India, TCI coaches ASHAs and ASHAs’ supervisors, Auxiliary Nurse Midwives, on how to systematically complete and use their urban health index register (UHIR) to prioritize household visits for FP counseling and use the logistics management system to restock short-term supplies like condoms and pills.
- In Francophone West Africa, TCI adapted India’s mapping and listing approach to its context and community relays play a critical role in conducting the mapping along with facility managers to identify women of reproductive age.
What Is the Evidence?
- The use of CHWs for family planning counseling and provision of methods increases contraceptive use. For a comprehensive yet succinct analysis of the evidence, see the High Impact Practices in Family Planning brief on CHWs.
- Allowing CHWs to provide condoms and oral contraceptives allows facility-based service providers more time to provide quality care in the facilities.
- In 2018 and 2019, CHWs and VHTs in East Africa referred over 42,000 clients for family planning services, with a 72% completion rate. They also distributed oral contraceptives to 29,815 clients in that same time period.
- As of November 2019, TCI in India reached 6,679 ASHAs with coaching support across its three supported states. ASHAs have become even more critical during COVID-19 lockdowns in reaching potential and existing FP clients with pills and condoms.
- Under URHI, women in India who were exposed to CHWs were significantly more likely to be modern contraceptive method users than women who did not recall any exposure.
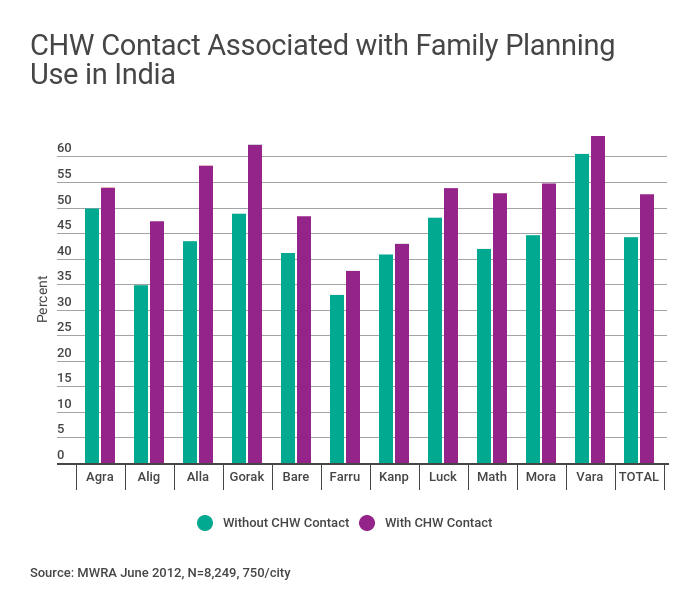
- In Uttar Pradesh, India, currently married fecund women with high exposure to CHWs were 1.59 times more likely to use a modern family planning method than women with no exposure to CHWs.

